
Long-term follow-up outcomes and salvage treatment strategy for recurrent neuroblastoma in children
-
摘要:
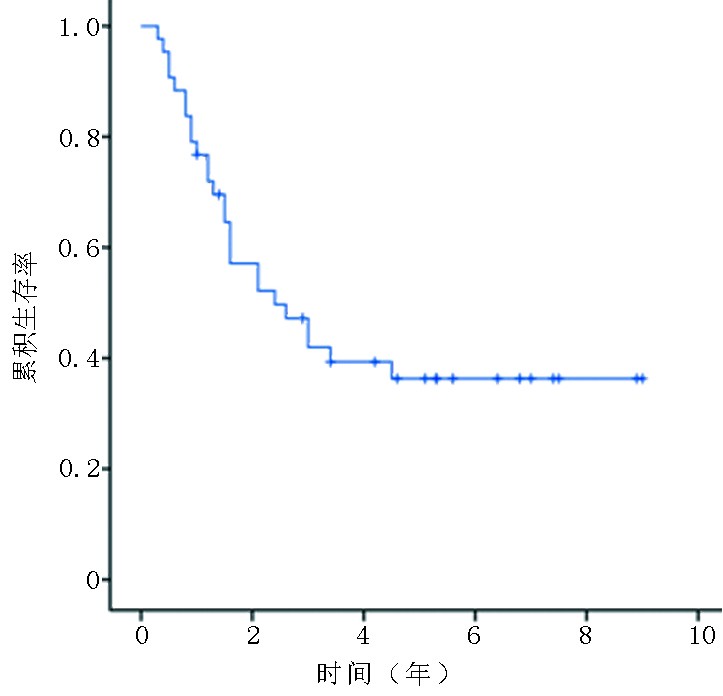
目的 分析儿童神经母细胞瘤(neuroblastoma,NB)复发的临床特点、生存情况,并对挽救治疗的策略进行讨论。 方法 回顾性分析2010年1月至2021年12月于上海交通大学医学院附属新华医院接受治疗后出现复发的43例NB患儿的复发类型、复发时间及初始治疗情况;通过生存分析、Cox多因素回归分析治疗失败的危险因素,并对挽救治疗的情况进行初步评价。 结果 共纳入43例复发儿童NB中,男女性别比2.1∶1,初发时中位诊断年龄为3.7(0.7~15.6)岁,复发时中位年龄为5.5(1.9~17.0)岁。9例患儿为局部复发,34例为多部位复发,主要累及部位包括骨骼、淋巴结、骨髓以及中枢神经系统。43例复发患儿中,1例初治为低危组、7例中危组,35例高危组。复发后经过再次治疗的随访中位时间为5.3年,截至末次随访时间有17例患儿处于生存状态,1、3、5年的总体生存率分别为(76.0±6.4)%、(42.0±7.8)%和(36.3±7.7)%。放疗的缺失是局部复发的危险因素(HR=2.3;95%CI:1.14~3.7)。局部复发后接受再次完整手术和放疗的患儿结局较好。VIT方案(长春新碱、伊立替康联合替莫唑胺)的血液学毒性显著低于其他挽救化疗方案。 结论 儿童NB的复发后挽救治疗需要根据复发类型、复发时间和初治情况等综合分析。VIT方案的毒性较低,疗效与其他方案相当,对复发NB的挽救治疗具有一定的价值。 Abstract:Objective To analyze the clinical characteristics and survival rates among children with recurrent neuroblastoma (NB) and to discuss the strategy of salvage treatment. Methods Recurrent NB cases enrolled between January 2010 and December 2021 at Xinhua Hospital Affiliated to Shanghai Jiao Tong University, School of Medicine were retrospectively analyzed by means of recurrence type, time to relapse, and initial treatment data. The risk factors for treatment failure were analyzed using survival analysis and a Cox multivariate regression model, and the strategy of salvage treatment was preliminarily evaluated. Results A total of 43 children with recurrent NB were enrolled in this single-center study. The male-to-female ratio was 2.1:1, and the median ages at the time of initial diagnosis and recurrence were 3.7 (0.7–15.6) years and 5.5 (1.9–17.0) years, respectively. Nine cases had local recurrence and 34 cases had multi-site recurrence, mainly involving the skeleton, lymph nodes, bone marrow, and central nervous system. Among the recurrent cases, one was initially treated in the low-risk group, seven in the medium-risk group, and 35 cases in the high-risk group. The median follow-up time after recurrence was 5.3 years, at which time 17 patients were still alive. The overall 1-year, 3-year, and 5-year survival rates were (76.0±6.4)%, (42.0±7.8)%, and (36.3±7.7)%, respectively. Absence of radiotherapy was a risk factor for local recurrence (HR=2.3; 95%CI: [1.14-3.7]). Patients with local recurrence had better outcomes after thorough excision and radiotherapy. The hematological toxicity of the vincristine, irinotecan, and temozolomide (VIT) regimen was significantly lower than that of other salvage chemotherapy regimens. Conclusions The salvage treatment for recurrent NB in children needs to be comprehensively analyzed according to the recurrence type and initial treatment. The toxicity of VIT regimen is low. The efficacy is comparable to other regimens, and it has a certain value for the salvage treatment of recurrent NB. -
Key words:
- neuroblastoma (NB) /
- children /
- recurrence/relapse /
- outcome
-
表 1 影响复发后NB患儿生存状态的因素分析
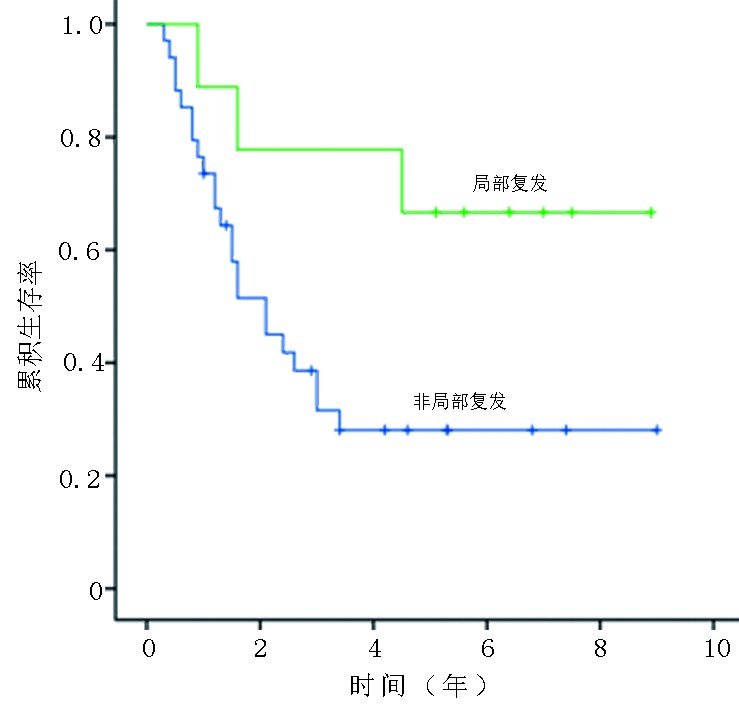
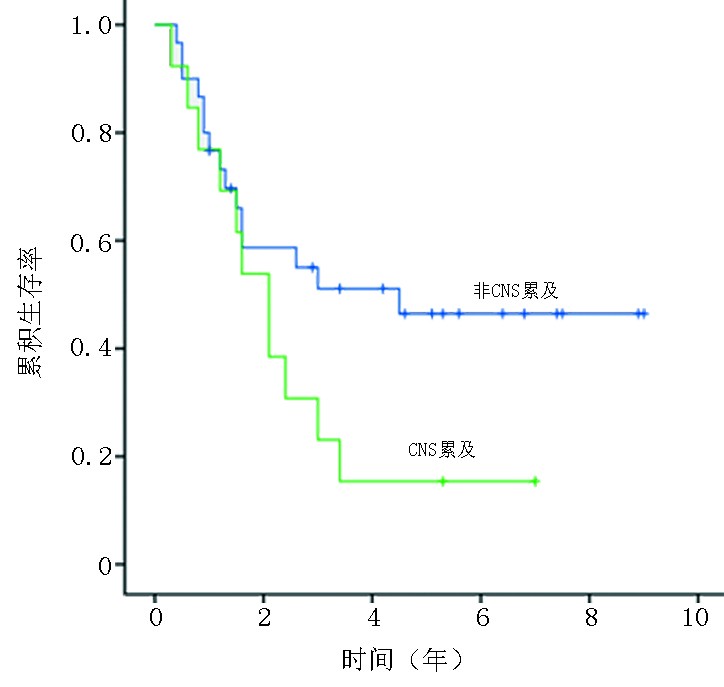
项目 例数 5年OS(%) χ2 P 复发类型 局部 9 66.7±15.7 4.185 0.041 非局部 34 28.1±8.1 复发距离初诊时间(月) <12 8 12.5±11.7 6.784 0.079 12~24 21 38.5±11.2 24~36 7 21.4±17.8 >36 7 71.4±17.1 复发累及CNS 累及 13 15.4±10.0 2.828 0.093 未累及 30 46.4±9.7 初治时规范治疗 是 22 27.3±9.5 2.598 0.107 否 21 47.0±11.7  下载: 导出CSV
下载: 导出CSV
表 2 初治因素对复发NB的多因素Cox回归分析
项目 例数 HR 95%CI P 局部未放疗 16 2.30 1.14~3.70 0.036 未行自体移植 33 1.23 0.76~1.35 0.250 未服用维甲酸 10 1.03 0.52~1.26 0.763
下载: 导出CSV
表 3 3种复发NB挽救化疗方案的有效性(客观反应率)和安全性分析(发生CTCAE Ⅳ级以上不良反应)
方案 例数 χ2 P 客观反应率 CTX+Topo 96/130 1.357 0.440 VIT 52/79 ICE 35/47 血液学毒性 CTX+TOPO 101/130 4.325 0.020 VIT 22/79 ICE 44/47 胃肠道毒性 CTX+TOPO 15/130 1.928 0.230 VIT 43/79 ICE 12/47
下载: 导出CSV
-
[1] Chung C, Boterberg T, Lucas J, et al. Neuroblastoma[J]. Pediatr Blood Cancer, 2021, 68(Suppl 2):e28473. [2] 中国抗癌协会小儿肿瘤专业委员会,中华医学会小儿外科学分会肿瘤外科学组.儿童神经母细胞瘤诊疗专家共识[J].中华小儿外科杂志,2015,36(1):3-7. [3] Irwin MS, Naranjo A, Zhang FF, et al. Revised neuroblastoma risk classification system: a report from the children’s oncology group[J]. J Clin Oncol, 2021, 39(29):3229-3241. doi: 10.1200/JCO.21.00278 [4] Li HF, Mao HJ, Zhao L, et al. The diagnostic accuracy of PET(CT) in patients with neuroblastoma: a meta-analysis and systematic review[J]. J Comput Assist Tomogr, 2020, 44(1):111-117. doi: 10.1097/RCT.0000000000000973 [5] Elzembely MM, Dahlberg AE, Pinto N, et al. Late effects in high-risk neuroblastoma survivors treated with high-dose chemotherapy and stem cell rescue[J]. Pediatr Blood Cancer, 2019, 66(1):e27421. doi: 10.1002/pbc.27421 [6] London WB, Frantz CN, Campbell LA, et al. Phase II randomized comparison of topotecan plus cyclophosphamide versus topotecan alone in children with recurrent or refractory neuroblastoma: a Children’s Oncology Group study[J]. J Clin Oncol, 2010, 28(24):3808-3815. doi: 10.1200/JCO.2009.27.5016 [7] Zhu J, Wang J, Sun FF, et al. Vincristine, irinotecan, and temozolomide in patients with relapsed/refractory neuroblastoma[J]. Front Oncol, 2022, 12:804310. doi: 10.3389/fonc.2022.804310 [8] Levy AS, Krailo M, Chi SS, et al. Temozolomide with irinotecan versus temozolomide, irinotecan plus bevacizumab for recurrent medulloblastoma of childhood: report of a COG randomized Phase II screening trial[J]. Pediatr Blood Cancer, 2021, 68(8):e29031. [9] Rosenberg AR, Orellana L, Kang TI, et al. Differences in parent-provider concordance regarding prognosis and goals of care among children with advanced cancer[J]. J Clin Oncol, 2014, 32(27):3005-3011. doi: 10.1200/JCO.2014.55.4659 [10] Zhang DD, Kaweme NM, Duan P, et al. Upfront treatment of pediatric high-risk neuroblastoma with chemotherapy, surgery, and radiotherapy combination: the CCCG-NB-2014 protocol[J]. Front Oncol, 2021, 11:745794. doi: 10.3389/fonc.2021.745794 [11] 中国抗癌协会小儿肿瘤专业委员会,中华医学会小儿外科学分会肿瘤学组.儿童神经母细胞瘤诊疗专家共识CCCG-NB-2021方案[J].中华小儿外科杂志,2022,43(7):588-598. [12] Mody R, Yu AL, Naranjo A, et al. Irinotecan, temozolomide, and dinutuximab with GM-CSF in children with refractory or relapsed neuroblastoma: a report from the children’s oncology group[J]. J Clin Oncol, 2020, 38(19):2160-2169. doi: 10.1200/JCO.20.00203 [13] GD单抗治疗神经母细胞瘤临床应用协作组,袁晓军,李杰,等.GD2抗体达妥昔单抗β治疗神经母细胞瘤的临床应用专家共识(2021年版)[J].临床儿科杂志,2022,40(1):14-20. -

 点击查看大图
点击查看大图
图(3) / 表(3)
计量
- 文章访问数: 112
- HTML全文浏览量: 24
- PDF下载量: 37
- 被引次数: 0
