
Surgical strategy for periacetabular metastases based on modified Harrington classification
-
摘要:
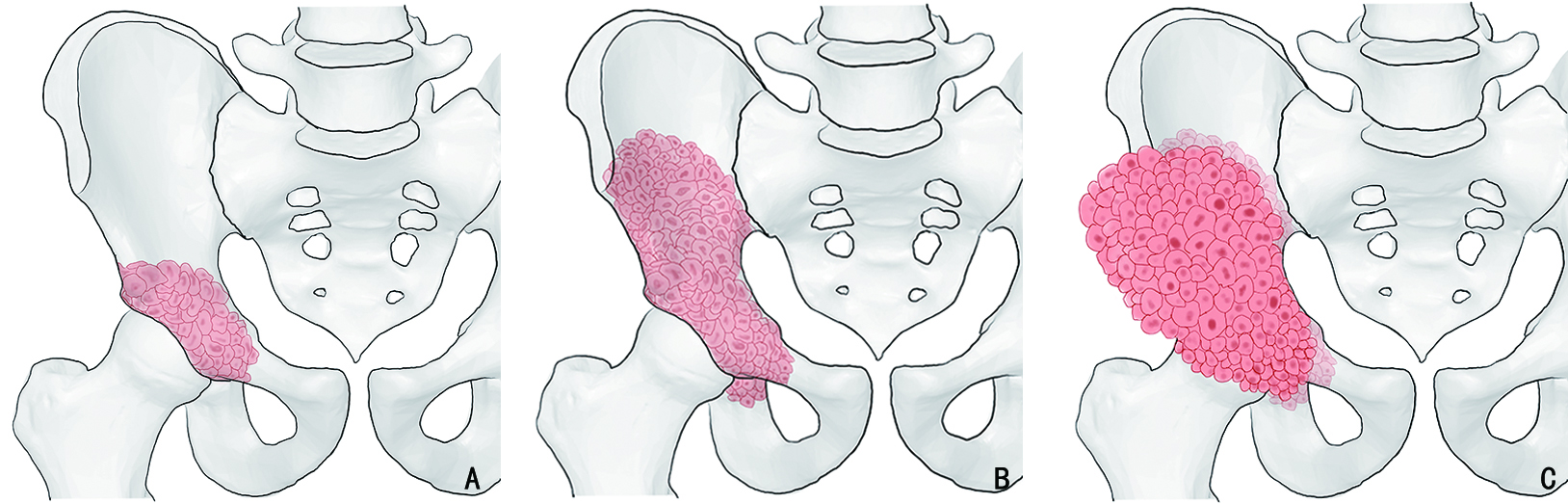
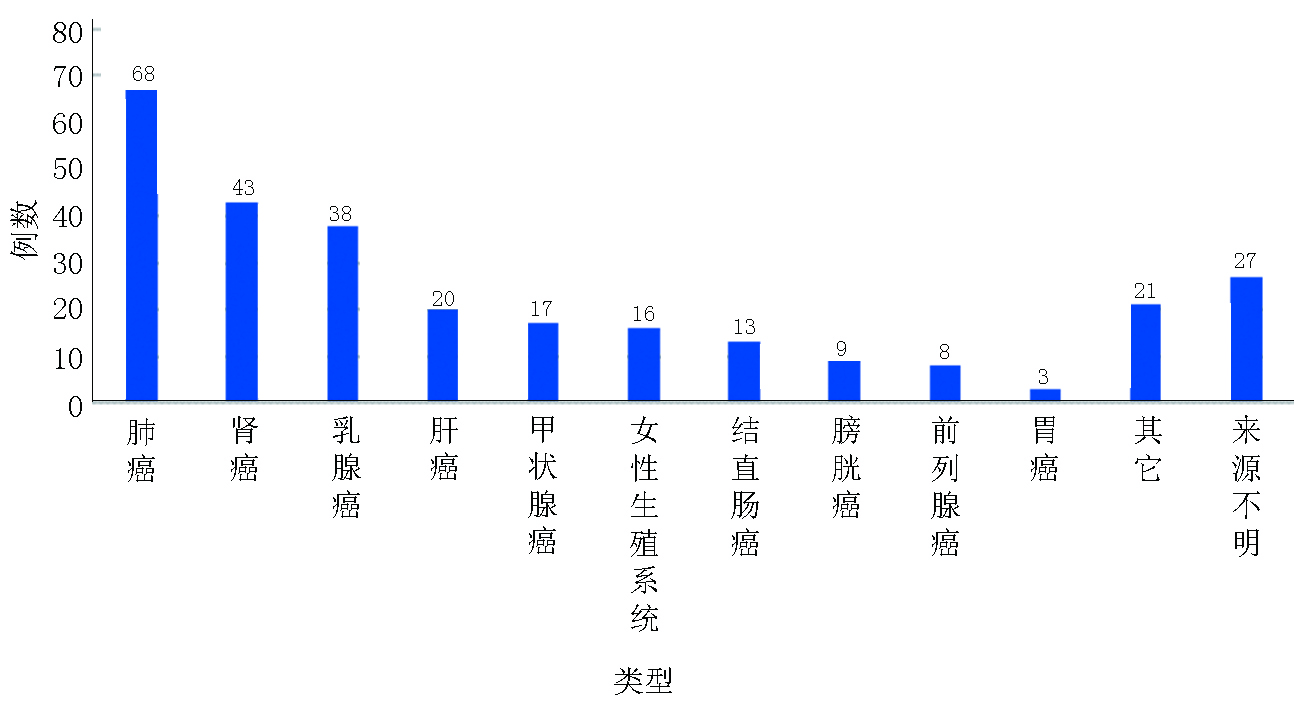
目的 对于髋臼转移癌的外科治疗方法尚缺乏统一的认识,本研究旨在提出了改良Harrington髋臼转移癌分型系统并基于此提出新的髋臼转移癌外科治疗策略。 方法 本研究回顾性选取2003年6月至2021年9月于北京大学人民医院行外科治疗的283例髋臼转移癌患者,其中男性146例、女性137例,平均年龄(56.2±12.4)岁。283例髋臼转移癌患者中最常见的病理类型为肺癌(68例)、肾癌(43例)与乳腺癌(38例)。北京大学人民医院骨与软组织肿瘤诊疗中心为针对性地规划髋臼转移癌的外科治疗方案,在传统Harrington分型的基础上对Ⅲ型病灶进行了细化分类,基于骨内病灶累及范围与软组织包块情况将其进一步分为Ⅲa型(骨破坏范围在骶髂关节平面以下且不伴巨大软组织肿块)、Ⅲb型(骨破坏范围超过骶髂关节平面以上且不伴巨大软组织肿块)与Ⅲc型(骨破坏伴巨大软组织肿块)。对Ⅲa病灶与部分Ⅲb病灶仍采用传统的瘤内手术联合斯氏针/空心钉骨水泥髋臼成型+全髋关节置换,而对于Ⅲc病灶与部分Ⅲb病灶则采用肿瘤整块切除联合假体重建。对Harrington Ⅰ、Ⅱ、Ⅳ型病灶患者的外科治疗仍按传统Harrington分型进行。 结果 283例患者中4例截肢,279例患者行基于改良外科分型系统的手术治疗。平均手术时间(218.6±82.4)min,平均出血量(1593.0 ± 1162.5)mL,围手术期并发症发生率为14.0%。术后随访期平均为(19.6±13.1)个月。术后MSTS 93功能评分平均(18.3±5.2)分,其中Harrington Ⅲ型髋臼周围转移癌中,采用斯氏针骨水泥髋臼成型+全髋置换患者术后MSTS93评分平均为(18.6±5.8)分,而采用肿瘤整块切除联合假体置换的患者术后MSTS93评分平均为(19.3±4.9)分。15例(5.3%)患者在生存期内出现肿瘤局部复发,其中4例为采取整块切除的病例,余11例均为刮除病例。 结论 对于骨盆转移癌导致严重疼痛和行走困难的患者,外科治疗可以缓解症状。本研究提出的改良Harrington外科分型能够有效地指导髋臼转移瘤外科治疗方案制定,在不增加手术风险的前提下具有针对性地提高了外科治疗的效果。 Abstract:Objective Periacetabular metastasis treatment remains diverse without a standard protocol. This study aimed to propose a novel surgical strategy for periacetabular metastases based on a modified Harrington classification. Methods We reviewed the data of 283 patients with periacetabular metastases who underwent surgeries at Peking University People’s Hospital from June 2003 to September 2021. There were 146 men and 137 women, and the mean age of the patients was (56.2±12.4) years. The most common histological diagnoses were metastatic lung cancer (68 cases), renal cancer (43 cases), and breast cancer (38 cases). A modified surgical classification for periacetabular metastases based on the Harrington classification was proposed. Surgeries were performed according to the original Harrington classification for patients with class I, Ⅱ, and Ⅳ lesions. For Harrington class Ⅲ lesions, three subtypes were further categorized based on the involvement of bone destruction and soft tissue mass volume; class Ⅲa lesions had bone destruction distal to the inferior border of the sacroiliac joint without giant soft tissue mass, class Ⅲb lesions had bone destruction extended proximally to the inferior border of the sacroiliac joint without a giant soft tissue mass, and class IIIc lesions had a giant soft tissue mass. Intralesional excision followed by the placement of Steinmann pins/screws with cemented total hip arthroplasty (THA) was performed for class Ⅲa and a few Ⅲb lesions, and en bloc resection followed by modular hemipelvic endoprosthesis replacement was performed for class Ⅲc lesions and the remaining Ⅲb lesions. Results Among 283 patients, 279 underwent limb salvage surgeries. All surgeries were completed uneventfully according to the proposed modified surgical classification. The mean surgical time was (218.6±82.4) min, and the mean intraoperative hemorrhage volume was (1593.0±1162.5) mL. Postoperative complications occurred in 14.0% of 279 patients. The mean follow-up period was (19.6±13.1) months. The mean Musculoskeletal Tumor Society (MSTS)-93 functional score was 18.3±5.2. Among patients with class Ⅲ lesions, the MSTS-93 scores of patients who underwent intralesional excision followed by placement of Steinmann pins/screws with cemented THA and en bloc resection followed by modular hemipelvic endoprosthesis replacement were 18.6±5.8 and 19.3±4.9, respectively. Recurrences were noted in 15 patients (5.3%), including four who underwent en bloc resection and 11 who underwent intralesional excision. Conclusions The indications for surgical interventions for pelvic metastasis are severe pain and difficulty in ambulation caused by metastatic lesions. According to our proposed modified Harrington classification, the outcomes of surgical treatment for patients with periacetabular metastases can be improved with no increased surgical risk. -
Key words:
- pelvic tumor /
- bone metastasis /
- surgical classification /
- reconstruction /
- surgery
-
表 1 Harrington髋臼转移癌外科分型[3]
分型 骨破坏情况 肿瘤清除方式 功能重建方式 Ⅰ 髋臼外侧壁、上方及内侧壁完好,累及关节面,病灶局限 瘤内手术 骨水泥THA Ⅱ 髋臼内侧壁缺损 瘤内手术 带翼网杯骨水泥THA Ⅲ 髋臼内壁、顶部及边缘均存在破坏 瘤内手术 斯氏针/空心钉骨水泥髋臼成型+THA Ⅳ 孤立髋臼转移 整块切除 假体重建  下载: 导出CSV
下载: 导出CSV
表 2 283例骨盆转移癌外科治疗资料
项目 例数 手术方式 保肢 279 截肢 4 Harrington分型 Ⅰ型 25 Ⅱ型 72 Ⅲ型 100 Ⅲa型 28 Ⅲb型 33 Ⅲc型 39 Ⅳ型 82 减少术中出血措施 术前选择性动脉栓塞 35 髂总/髂外动脉临时阻断 48 腹主动脉球囊临时阻断 86
下载: 导出CSV
-
[1] Shahid M, Saunders T, Jeys L, et al. The outcome of surgical treatment for peri-acetabular metastases[J]. Bone Joint J, 2014, 96(1):132-136. [2] Issack PS, Kotwal SY, Lane JM. Management of metastatic bone disease of the acetabulum[J]. J Am Acad Orthop Surg, 2013, 21(11):685-695. [3] Harrington KD. The management of acetabular insufficiency secondary to metastatic malignant disease[J]. J Bone Joint Surg Am, 1981, 63(4):653-664. doi: 10.2106/00004623-198163040-00017 [4] Hoshi M, Taguchi S, Takada J, et al. Palliative surgery for acetabular metastasis with pathological central dislocation of the hip joint after radiation therapy: a case report[J]. Jpn J Clin Oncol, 2012, 42(8):757-760. doi: 10.1093/jjco/hys071 [5] Tillman R, Tsuda Y, Veettil MP, et al. The long-term outcomes of modified Harrington procedure using antegrade pins for periacetabular metastasis and haematological diseases[J]. The bone & Joint Journal, 2019, 101(12):1557-1562. [6] Yang R, Goch A, Murphy D, et al. A novel tripod percutaneous reconstruction technique in periacetabular lesions caused by metastatic cancer[J]. J Bone Joint Surg Am, 2020, 102(7):592-599. doi: 10.2106/JBJS.19.00936 [7] Ji T, Guo W, Yang RL, et al. Clinical outcome and quality of life after surgery for peri-acetabular metastases[J]. Journal of Bone and Joint Surgery, 2011, 93(8):1104-1110. [8] Ho L, Ahlmann ER, Menendez LR. Modified Harrington reconstruction for advanced periacetabular metastatic disease[J]. J Surg Oncol, 2010, 101(2):170-174. doi: 10.1002/jso.21440 [9] Guo W, Li D, Tang X, et al. Reconstruction with modular hemipelvic prostheses for periacetabular tumor[J]. Clin Orthop Relat Res, 2007, 461:180-188. doi: 10.1097/BLO.0b013e31806165d5 [10] Benevenia J, Cyran FP, Biermann JS, et al. Treatment of advanced metastatic lesions of the acetabulum using the saddle prosthesis[J]. Clin Orthop Relat Res, 2004(426):23-31. [11] Maccauro G, Liuzza F, Scaramuzzo L, et al. Percutaneous acetabuloplasty for metastatic acetabular lesions[J]. BMC Musculoskelet Disord, 2008, 9:66. doi: 10.1186/1471-2474-9-66 [12] Tang XD, Guo W, Yang RL, et al. Evaluation of blood loss during limb salvage surgery for pelvic tumours[J]. Int Orthop, 2009, 33(3):751-756. [13] Enneking WF, Dunham W, Gebhardt MC, et al. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system[J]. Clin Orthop Relat Res, 1993(286):241-246. [14] Kunisada T, Choong PF. Major reconstruction for periacetabular metastasis: early complications and outcome following surgical treatment in 40 hips[J]. Acta Orthop Scand, 2000, 71(6):585-590. [15] Tang X, Guo W, Ji T. Reconstruction with modular hemipelvic prosthesis for the resection of solitary periacetabular metastasis[J]. Arch Orthop Trauma Surg, 2011, 131(12):1609-1615. doi: 10.1007/s00402-011-1359-5 [16] Ruggieri P, Mavrogenis AF, Angelini A, et al. Metastases of the pelvis: does resection improve survival[J]? Orthopedics, 2011, 34(7):e236-e244. [17] Kim HS, Kim KJ, Han I, et al. The use of pasteurized autologous grafts for periacetabular reconstruction[J]. Clin Orthop Relat Res, 2007, 464:217-223. doi: 10.1097/BLO.0b013e3181583ae4 [18] Bus MP, Szafranski A, Sellevold S, et al. LUMiC® endoprosthetic reconstruction after periacetabular tumor resection: short-term results[J]. Clin Orthop Relat Res, 2017, 475(3):686-695. doi: 10.1007/s11999-016-4805-4 [19] Ji T, Yang Y, Tang X, et al. 3D-Printed Modular Hemipelvic Endoprosthetic Reconstruction Following Periacetabular Tumor Resection: Early Results of 80 Consecutive Cases[J]. J Bone Joint Surg Am, 2020, 102(17):1530-1541. doi: 10.2106/JBJS.19.01437 -

 点击查看大图
点击查看大图
图(5) / 表(2)
计量
- 文章访问数: 137
- HTML全文浏览量: 95
- PDF下载量: 27
- 被引次数: 0
