
Expression levels and clinical significance of serum inflammatory cytokines andmyeloid-derived suppressor cells in patients with pulmonary ground-glass nodule
-
摘要:
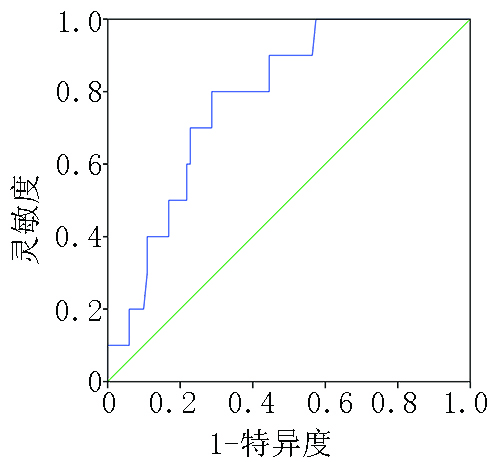
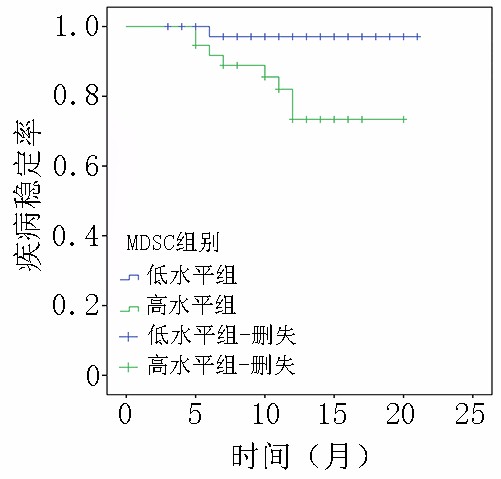
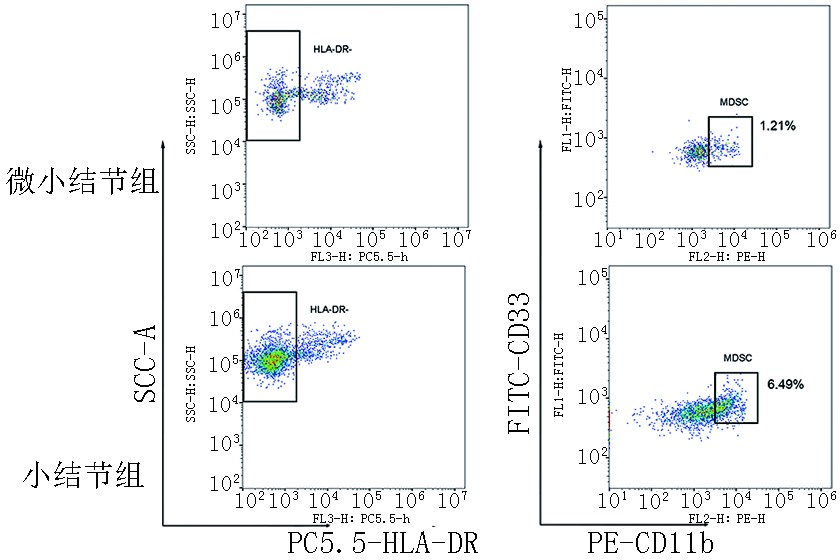
目的 探究血清炎症因子及外周血髓源性抑制细胞(myeloid-derived suppressor cells,MDSCs)在直径≤1 cm的肺磨玻璃结节(ground-glass nodule,GGN)患者中的表达,分析可能影响肺结节大小及进展的临床指标和意义。 方法 采用前瞻性研究方法纳入2020年4月至2021年7月就诊于上海中医药大学附属市中医医院肺GGN直径≤1 cm的患者111例,根据肺结节大小分为微小结节组(直径<5 mm)、小结节组(直径为5~10 mm),其中微小结节组36例,小结节组75例。检测各组患者血清炎症因子表达以及外周血髓源性抑制细胞的比例,分析组间差异。后续每半年随访1次,以影像学显示肺GGN直径增大2 mm及以上或出现新的GGN为研究终点,分析可能影响肺GGN进展的危险因素。 结果 小结节组较微小结节组患者MDSCs的比例升高,差异具有统计学意义(P<0.05),两组间炎症因子白细胞介素-2(interleukin-2,IL-2)、白细胞介素-6(interleukin-6,IL-6)、白细胞介素-8(interleukin-8,IL-8)和肿瘤坏死因子-α(tumor necrosis factor-α,TNF-α)表达差异无统计学意义(P>0.05)。两组间肺结节变化率差异无统计学意义(P>0.05)。MDSCs是影响肺GGN进展的危险因素,差异具有统计学意义(P<0.05),根据MDSCs表达水平的截断值进行分组分析,结果显示MDSCs低水平表达组(MDSCs<4.57%)较高水平表达组(MDSCs≥4.57%)疾病稳定期更长,差异具有统计学意义(P=0.001)。 结论 MDSCs表达水平与肺GGN大小相关,可能是影响肺GGN进展的因素之一。 Abstract:Objective To assess the expression of serum inflammatory cytokines and proportion of peripheral blood myeloid-derived suppressor cells (MDSCs) in patients with ground-glass nodule (GGN) ≤1 cm in diameter and analyze clinical indicators that may affect the size and progression of pulmonary nodules and their clinical significance. Methods This prospective study included 111 patients with pulmonary GGNs ≤1 cm in diameter who were admitted to Shanghai Municipal Hospital of Traditional Chinese Medicine from April 2020 to July 2021. Based on pulmonary nodule size, 36 and 75 patients were assigned into minute nodule (diameter <5 mm) and small nodule (diameter 5–10 mm) groups, respectively. The expression of inflammatory cytokines and proportion of MDSCs were determined, and the differences between the groups were analyzed. Follow-up visits were conducted every 6 months. The study endpoint was an increase in pulmonary GGN diameter of ≥2 mm or the occurrence of new GGNs. Risk factors that could affect the progression of pulmonary GGNs were also analyzed. Results The proportion of MDSCs was higher in the small nodule group than in the minute nodule group, with the difference being significant (P<0.05). Interleukin-2 (IL-2), interleukin-6 (IL-6), interleukin-8 (IL-8), and tumor necrosis factor-α (TNF-α) expressions were not significantly different between the two groups (P>0.05). There was no significant difference in the change rate of pulmonary nodules between the two groups (P>0.05). The proportion of MDSCs was a risk factor that affected the progression of pulmonary GGNs, and the difference was statistically significant (P<0.05). Based on the cutoff proportion of MDSCs, the duration of stable disease stage was longer in the low-proportion MDSCs group (MDSCs <4.57%) than in the high-proportion MDSCs expression group (MDSCs≥4.57%), and the difference was statistically significant (P=0.001). Conclusions The proportion of MDSCs is correlated with the size of pulmonary GGNs, which may be one of the factors affecting the progression of pulmonary GGNs. -
表 1 两组患者一般临床资料比较
项目 微小结节组(n=36) 小结节组(n=75) χ2/F P 性别 0.405a 0.527 男 11 29 女 25 46 年龄(岁) 54.17±14.49 55.40±13.17 1.628b 0.205 吸烟史 0.936a − 有 5 10 无 31 65 家族史 0.929a 1.000 有 6 12 无 30 63 结节数量 0.116a 0.137 孤立性 16 22 多发性 20 53 a:χ2值,b:F值  下载: 导出CSV
下载: 导出CSV
表 2 两组间炎症因子及MDSCs表达水平比较
项目 微小结节组(n=36) 小结节组(n=75) F/Z P IL-2 333.89±105.68 322.80±100.28 0.112b 0.593 IL-6 1.52(1.09) 2.08(1.30) −1.603c 0.109 IL-8 8.30(6.10) 7.27(4.76) −0.624c 0.533 TNF-α 6.15(3.72) 5.88(2.00) −1.841c 0.066 MDSCs(%) 2.56(2.50) 3.63(5.44) −1.997c 0.046 b:F值,c:Z值
下载: 导出CSV
表 3 两组间肺GGN变化率比较
结节变化 微小结节组(n=36) 小结节组(n=75) P 稳定 33(8.33) 68(9.33) 0.585 增大/增多 3(91.67) 7(90.67) − ()内单位为%
下载: 导出CSV
表 4 肺GGN单因素分析
参数 结节稳定 结节增大 OR 95%CI P 下限 上限 结节大小(mm) 1.132 0.275 4.661 0.863 <5 33(91.67) 3(8.33) 5~10 68(90.67) 7(9.33) 结节数量 0.451 0.091 2.24 0.331 孤立性 36(89.74) 2(5.26) 多发性 65(89.00) 8(11.00) 吸烟史 1.692 0.323 8.859 0.533 否 88(91.67) 8(8.33) 是 13(86.67) 2(13.33) 家族史 0.549 0.065 4.623 0.581 否 84(90.32) 9(9.68) 是 17(94.44) 1(5.56) IL-2 − − 0.975 0.948 1.004 0.086 IL-6 − − 0.806 0.432 1.503 0.497 IL-8 − − 0.877 0.672 1.143 0.331 TNF-α − − 2.065 0.666 6.409 0.209 MDSCs(%) − − 1.728 1.009 2.957 0.046 ()内单位为%
下载: 导出CSV
表 5 不同MDSCs表达水平对肺GGN进展的影响分析
MDSCs分组 疾病稳定期(月) χ2 P 低水平表达组 20.565±0.303 11.372 0.001 高水平表达组 17.075±0.907 − −
下载: 导出CSV
-
[1] 张晓菊,白莉,金发光,等.肺结节诊治中国专家共识(2018年版)[J].中华结核和呼吸杂志,2018,41(10):763-771. doi: 10.3760/cma.j.issn.1001-0939.2018.10.004 [2] Kim HY, Shim YM, Lee KS, et al. Persistent pulmonary nodular ground-glass opacity at thin-section CT: histopathologic comparisons[J]. Radiology, 2007, 245(1):267-275. doi: 10.1148/radiol.2451061682 [3] 田龙,沈诚,车国卫.肺部磨玻璃密度影研究进展[J].中国胸心血管外科临床杂志,2015,22(4):371-374. doi: 10.7507/1007-4848.20150098 [4] Jin CC, Lagoudas GK, Zhao C, et al. Commensal microbiota promote lung cancer development via γδ T cells[J]. Cell, 2019, 176(5):998-1013. [5] Bronte V, Brandau S, Chen SH, et al. Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards[J]. Nat Commun, 2016, 7:12150. doi: 10.1038/ncomms12150 [6] Bergenfelz C, Larsson AM, von Stedingk K, et al. Systemic monocytic-MDSCs are generated from monocytes and correlate with disease progression in breast cancer patients[J]. PLoS One, 2015, 10(5):e0127028. doi: 10.1371/journal.pone.0127028 [7] Yamauchi Y, Safi S, Blattner C, et al. Circulating and tumor myeloid-derived suppressor cells in resectable non-small cell lung cancer[J]. Am J Respir Crit Care Med, 2018, 198(6):777-787. doi: 10.1164/rccm.201708-1707OC [8] 中国物联网辅助评估管理肺结节专家组.物联网辅助评估管理肺结节中国专家共识[J].国际呼吸杂志,2022,42(1):5-12. doi: 10.3760/cma.j.cn131368-20211110-00835 [9] Mazzone PJ, Lam L. Evaluating the patient with a pulmonary nodule: a review[J]. JAMA, 2022, 327(3):264-273. doi: 10.1001/jama.2021.24287 [10] Nasim F, Ost DE. Management of the solitary pulmonary nodule[J]. Curr Opin Pulm Med, 2019, 25(4):344-353. doi: 10.1097/MCP.0000000000000586 [11] Jonas DE, Reuland DS, Reddy SM, et al. Screening for lung cancer with low-dose computed tomography: updated evidence report and systematic review for the US preventive services task force[J]. JAMA, 2021, 325(10):971-987. doi: 10.1001/jama.2021.0377 [12] Heuvelmans MA, Walter JE, Peters RB, et al. Relationship between nodule count and lung cancer probability in baseline CT lung cancer screening: the NELSON study[J]. Lung Cancer, 2017, 113:45-50. doi: 10.1016/j.lungcan.2017.08.023 [13] 钟文英,林秋娥,王黎平,等.健康体检人群肺部结节发生的影响因素分析[J].福建医药杂志,2019,41(2):140-142. doi: 10.3969/j.issn.1002-2600.2019.02.053 [14] 潘越,江启成.健康体检人群肺结节检出情况及影响因素分析[J].预防医学情报杂志,2020,36(3):356-359. [15] Li XF, Ren F, Wang SH, et al. The epidemiology of ground glass opacity lung adenocarcinoma: a network-based cumulative meta-analysis[J]. Front Oncol, 2020, 10:1059. doi: 10.3389/fonc.2020.01059 [16] Gabrilovich DI. Myeloid-derived suppressor cells[J]. Cancer Immunol Res, 2017, 5(1):3-8. doi: 10.1158/2326-6066.CIR-16-0297 [17] Hegde S, Leader AM, Merad M. MDSC: markers, development, states, and unaddressed complexity[J]. Immunity, 2021, 54(5):875-884. [18] Zhou J, Nefedova Y, Lei AH, et al. Neutrophils and PMN-MDSC: their biological role and interaction with stromal cells[J]. Semin Immunol, 2018, 35:19-28. doi: 10.1016/j.smim.2017.12.004 [19] Weber R, Groth C, Lasser S, et al. IL-6 as a major regulator of MDSC activity and possible target for cancer immunotherapy[J]. Cell Immunol, 2021, 359:104254. doi: 10.1016/j.cellimm.2020.104254 [20] Shi J, Liu X, Ming ZJ, et al. Value of combined detection of cytokines and tumor markers in the Differential diagnosis of benign and malignant solitary pulmonary nodules[J]. Chin J Lung Cancer, 2021, 24(6):426-433. [21] Liu CY, Xie WG, Wu S, et al. A comparative study on inflammatory factors and immune functions of lung cancer and pulmonary ground-glass attenuation[J]. Eur Rev Med Pharmacol Sci, 2017, 21(18):4098-4103. -

 点击查看大图
点击查看大图
图(3) / 表(5)
计量
- 文章访问数: 133
- HTML全文浏览量: 32
- PDF下载量: 26
- 被引次数: 0
