
-
摘要:
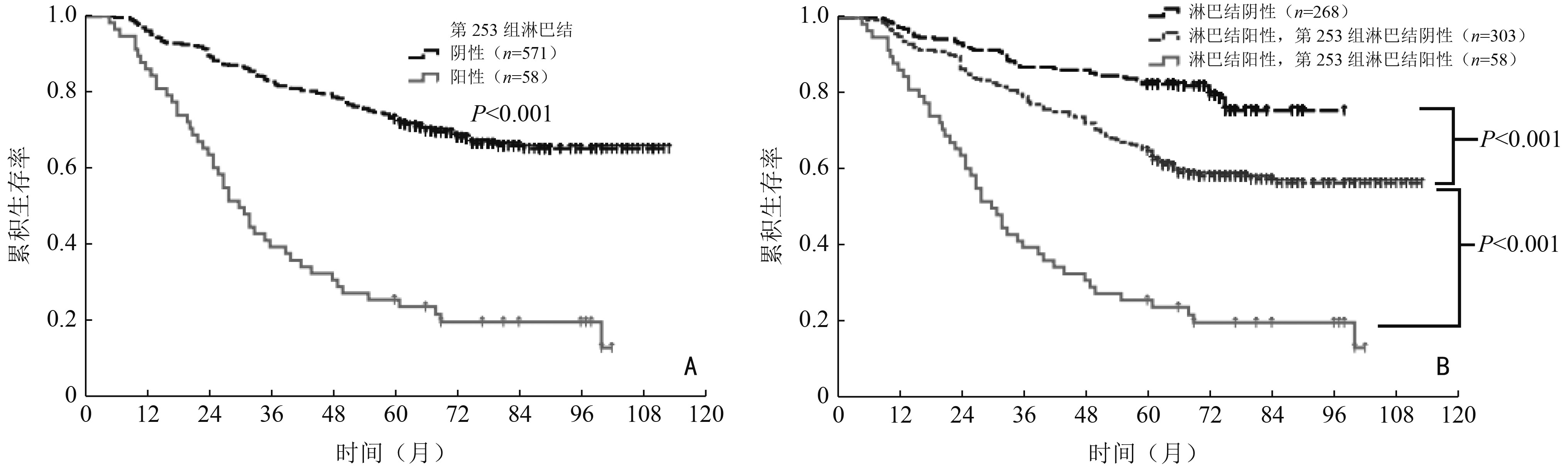
目的 探讨左半结肠癌第253组淋巴结转移及清扫的临床价值。 方法 回顾性收集2009年1月至2015年12月于海南医学院第二附属医院和海南医学院第一附属医院收治的629例左半结肠癌患者的临床病理资料,分析影响第253组淋巴结转移的临床病理因素及其与预后的关系。 结果 629例患者中58例(9.2%)有第253组淋巴结转移。肿瘤部位、pT分期、pN分期、癌结节、脉管癌栓和术前CA19-9水平与第253组淋巴结转移独立相关。分层分析显示,第253组淋巴结转移对pN1、pN2a和pN2b期患者预后影响均具有统计学意义。单因素生存分析显示,Ⅲ期左半结肠癌第253组淋巴结转移和未转移患者5年生存率分别为25.9%和65.0%,差异具有统计学意义(P<0.001)。倾向匹配后进行多因素生存分析,证实第253组淋巴结转移是Ⅲ期左半结肠癌患者的独立预后因素(HR=1.474,95%CI:1.072~2.498;P=0.037)。 结论 第253组淋巴结转移是Ⅲ期左半结肠癌患者的独立预后因素,第253组淋巴结状态对肿瘤分期、预后评估具有重要意义,存在该组淋巴结转移的患者预后不良。 Abstract:Objective To investigate the clinical value of No.253 lymph node metastasis and dissection in left hemi-colon cancer. Methods A total of 629 patients with left hemi-colon cancer from The Second Affiliated Hospital and The First Affiliated Hospital of Hainan Medical University, between January 2009 and December 2015, were enrolled. Clinicopathological factors correlating with No.253 lymph node metastasis and potential prognostic factors were analyzed. Results Fifty-eight (9.2%) patients had No.253 lymph node metastases. In multivariate analyses, tumor location, pT stage, pN stage, extranodal tumor deposits, lymphovascular invasion, and preoperative CA19-9 levels were independent risk factors for No.253 lymph node metastasis. Stratified analyses revealed that No.253 lymph node metastasis had a negative impact on overall survival in patients with pN1, pN2a, and pN2b stage disease. Five-year overall survival rates were 25.9% and 65.0% for those with stage Ⅲ disease with and without No.253 lymph node metastasis, respectively, and the survival difference was significant (P <0.001). After propensity score matching, multivariate survival analysis confirmed that No.253 lymph node metastasis was an independent prognostic factor in patients with stage Ⅲ left hemi-colon cancer (HR=1.474, 95%CI:1.072-2.498; P=0.037). Conclusions No.253 lymph node metastasis was an independent prognostic factor in patients with stage Ⅲ left hemi-colon cancer. The status of the No.253 lymph node plays an important role in stage and prognosis evaluations. Patients with No.253lymph node metastasis had a poorer prognosis. -
Key words:
- left hemi-colon cancer /
- No.253 lymph node /
- risk factors /
- prognosis
-
表 1 第253组淋巴结转移与左半结肠癌临床病理因素的关系
临床病理特征 第253组淋巴结例数(n=629) χ2 P 阴性(n=571) 阳性(n=58) 性别 0.792 0.373 男 330(91.7) 30(8.3) 女 241(89.6) 28(10.4) 年龄(岁) 0.312 0.577 <65 404(91.2) 39(8.8) ≥65 167(89.8) 19(10.2) 肿瘤部位 10.680 0.001 降结肠 286(94.7) 16(5.3) 乙状结肠 285(87.2) 42(12.8) 肿瘤大小(cm) 5.834 0.016 <5 282(93.7) 19(6.3) ≥5 289(88.1) 39(11.9) 组织学 6.910 0.009 高、中分化 184(95.3) 9(4.7) 低分化及未分化 387(88.8) 49(11.2) pT分期(期) 10.377 0.035 pT1 10(100.0) 0(0) pT2 59(95.2) 3(4.8) pT3 166(93.8) 11(6.2) pT4a 314(89.2) 38(10.8) pT4b 22(78.6) 6(21.4) pN分期(期) 68.169 <0.001 pN0 268(100.0) 0(0) pN1 186(88.6) 24(11.4) pN2a 97(80.8) 23(19.2) pN2b 20(64.5) 11(35.5) 癌结节 14.380 <0.001 无 528(92.1) 45(7.9) 有 43(76.8) 13(23.2) 脉管癌栓 22.677 <0.001 无 520(92.7) 41(7.3) 有 51(75.0) 17(25.0) 神经浸润 6.154 0.013 无 507(91.8) 45(8.2) 有 64(83.1) 13(16.9) 术前CEA 9.333 0.002 正常 354(93.7) 24(6.3) 升高 217(86.5) 34(13.5) 术前CA19-9 20.583 <0.001 正常 475(93.3) 34(6.7) 升高 96(80.0) 24(20.0) ( )内单位为%  下载: 导出CSV
下载: 导出CSV
表 2 影响第253组淋巴结转移的多因素分析
临床病理因素 HR 95% CI P 肿瘤部位(乙状结肠 vs. 降结肠) 2.530 1.200~5.333 0.015 肿瘤大小(≥5 cm vs. <5 cm) 1.287 0.635~2.609 0.485 组织学(低分化及未分化 vs. 高、中分化) 1.974 0.757~5.149 0.165 pT分期(pT4a~4b vs. pT1~3) 3.617 1.396~9.370 0.008 pN分期(pN2b~2a vs. pN0~1) 2.789 1.982~3.925 <0.001 癌结节(有 vs. 无) 3.385 1.404~8.161 0.007 脉管癌栓(有 vs. 无) 13.134 5.028~34.310 <0.001 神经侵犯(有 vs. 无) 2.145 0.948~4.855 0.067 术前CEA(升高 vs. 正常) 1.035 0.504~2.126 0.925 术前CA19-9(升高 vs. 正常) 4.072 1.853~8.949 <0.001
下载: 导出CSV
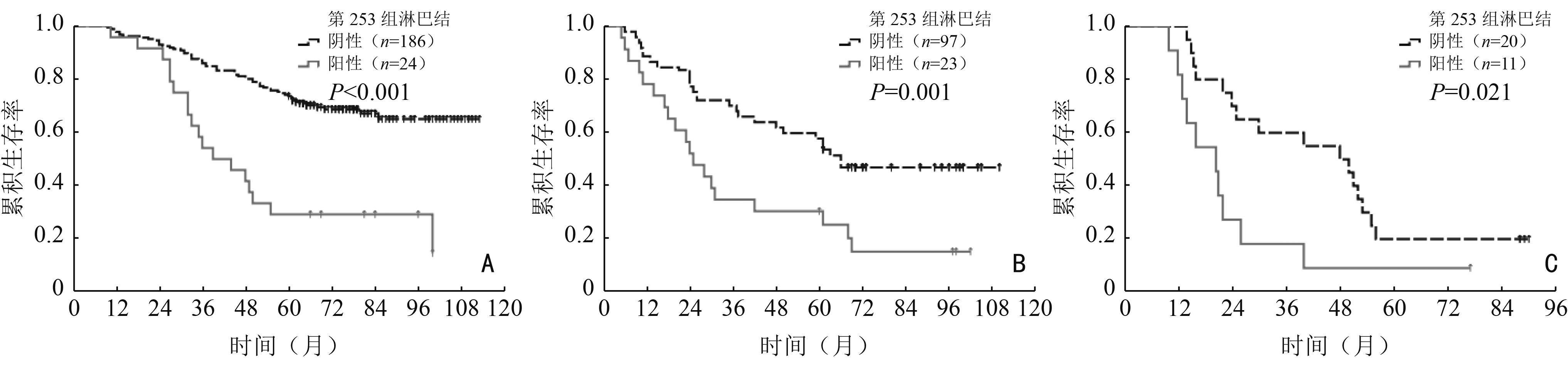
表 3 分层分析第253组淋巴结转移对不同N分期左半结肠癌患者预后影响
pN分期 第253组淋巴结阴性 第253组淋巴结阳性 χ2 P 例数(例) 5年生存率 (%) 例数(例) 5年生存率 (%) pN0 268 82.5 − − − − pN1 186 73.7 24 29.2 24.201 <0.001 pN2a 97 57.7 23 30.4 11.351 0.001 pN2b 20 20.0 11 9.1 5.288 0.021
下载: 导出CSV
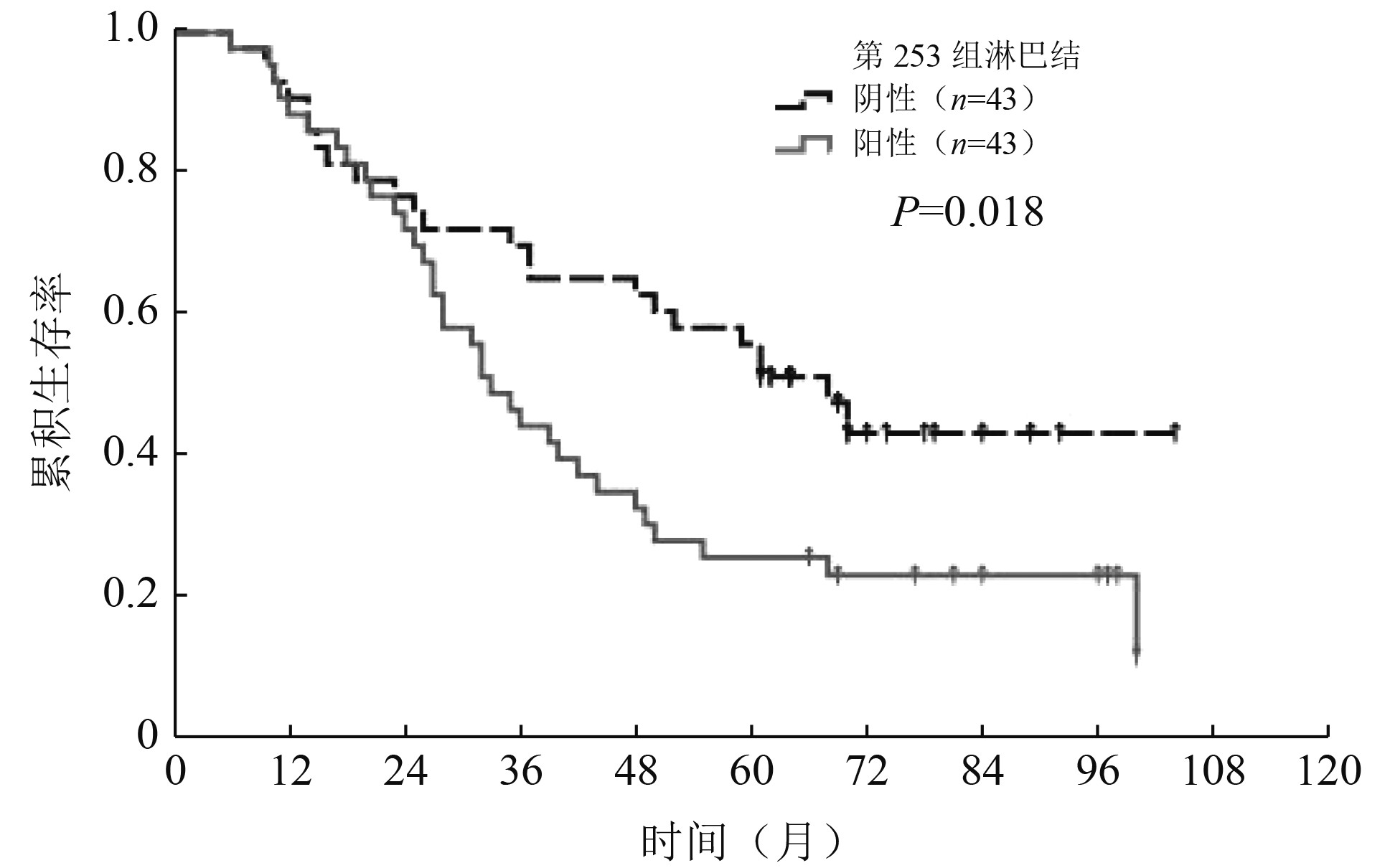
表 4 Ⅲ期左半结肠癌患者倾向匹配前后临床病理特征比较
临床病理特征 倾向匹配前(n=361) 倾向匹配后(n=86) 第253组淋巴结阴性(n=303) 第253组淋巴结阳性(n=58) χ2 P 第253组淋巴结阴性(n=43) 第253组淋巴结阳性(n=43) χ2 P 性别 0.029 0.864 0.420 0.517 男 153(83.6) 30(16.4) 19(46.3) 22(53.7) 女 150(84.3) 28(15.7) 24(53.3) 21(46.7) 年龄(岁) 0.452 0.501 3.087 0.079 <65 217(84.8) 39(15.2) 36(55.4) 29(44.6) ≥65 86(81.9) 19(18.1) 7(33.3) 14(66.7) 肿瘤部位 7.112 0.008 0.000 1.000 降结肠 141(89.8) 16(10.2) 13(50.0) 13(50.0) 乙状结肠 162(79.4) 42(20.6) 30(50.0) 30(50.0) 肿瘤大小(cm) 2.125 0.145 0.221 0.639 <5 125(87.4) 18(12.6) 12(46.2) 14(53.8) ≥5 178(81.7) 40(18.3) 31(51.7) 29(48.3) 组织学 4.342 0.037 3.528 0.060 高、中分化 87(90.6) 9(9.4) 17(65.4) 9(34.6) 低分化及未分化 216(81.5) 49(18.5) 26(43.3) 34(56.7) pT分期(期) 4.653 0.325 5.590 0.133 pT1 2(100.0) 0(0.0) − − pT2 38(82.6) 3(17.4) 6(46.2) 7(53.8) pT3 55(90.2) 11(9.8) 9(69.2) 4(30.8) pT4a 189(84.4) 38(15.6) 27(50.9) 26(49.1) pT4b 19(67.9) 6(32.1) 1(14.3) 6(85.7) pN分期(期) 12.872 0.002 1.517 0.468 pN1 186(88.6) 24(11.4) 26(53.1) 23(46.9) pN2a 97(80.8) 23(19.2) 10(40.0) 15(60.0) pNb 20(64.5) 11(35.5) 7(58.3) 5(41.7) 癌结节 7.264 0.007 0.796 0.372 无 273(85.8) 45(14.2) 25(46.3) 29(53.7) 有 30(69.8) 13(30.2) 18(56.3) 14(43.8) 脉管癌栓 35.759 <0.001 0.281 0.596 无 288(87.5) 41(12.5) 35(51.5) 33(48.5) 有 15(46.9) 17(53.1) 8(44.4) 10(55.6) 神经浸润 4.247 0.039 2.529 0.112 无 266(85.5) 45(14.5) 37(54.4) 31(45.6) 有 37(74.0) 13(26.0) 6(33.3) 12(66.7) 术前CEA 7.462 0.006 1.173 0.279 正常 184(88.5) 24(11.5) 26(55.3) 21(44.7) 升高 119(77.8) 34(22.2) 17(43.6) 22(56.4) 术前CA19-9 13.713 <0.001 0.205 0.651 正常 245(87.8) 34(12.2) 29(51.8) 27(48.2) 升高 58(70.7) 24(29.3) 14(46.7) 16(53.3) 手术方式 1.769 0.184 3.018 0.082 腹腔镜 149(86.6) 23(13.4) 23(60.5) 15(39.5) 开腹 154(81.5) 35(18.5) 20(41.7) 28(58.3) 术后并发症 29.813 <0.001 0.341 0.559 无 293(86.7) 45(13.3) 37(51.4) 35(48.6) 有 10(43.5) 13(56.5) 6(42.9) 8(57.1) 术后辅助化疗 0.002 0.968 0.156 0.693 无 36(83.7) 7(16.3) 3(42.9) 4(57.1) 有 267(84.0) 51(16.0) 40(50.6) 39(49.4) ( )内单位为%
下载: 导出CSV
表 5 Ⅲ期左半结肠癌患者倾向匹配后多因素预后分析
临床病理因素 HR 95% CI P pN分期(N2 vs. N1) 1.282 1.036-1.586 0.022 癌结节(有 vs. 无) 1.714 0.9812.994 0.058 术前CEA(正常 vs. 升高) 1.600 0.889-2.879 0.117 术前CA19-9(正常 vs. 升高) 1.732 1.018-2.948 0.043 术后辅助化疗(无 vs. 有) 3.061 1.362-6.879 0.007 第253组淋巴结(阳性 vs. 阴性) 1.474 1.072-2.498 0.037
下载: 导出CSV
-
[1] National health commission of the people's republic of China. National guidelines for diagnosis and treatment of colorectal cancer 2020 in China (English version)[J]. Chin J Cancer Res, 2020, 32(4):415-445. doi: 10.21147/j.issn.1000-9604.2020.04.01 [2] Hashiguchi Y, Muro K, Saito Y, et al. Japanese society for cancer of the colon and rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer[J]. Int J Clin Oncol, 2020, 25(1):1-42. doi: 10.1007/s10147-019-01485-z [3] Zhao X, Ma JJ, Fu ZW, et al. Prognostic value of apical lymph node metastasis at the inferior mesenteric artery in sigmoid and rectal cancer patients who undergo laparoscopic surgery[J]. J Surg Oncol, 2021, 123(Suppl 1): S88-S94. [4] Zhou SJ, Shen Y, Huang C, et al. Prognosis of patients with colorectal cancer and apical lymph node metastasis at the inferior mesenteric artery: a systematic review and Meta-analysis[J]. Front Med (Lausanne), 2021, 8:800717. [5] Takabatake K, Arita T, Nakanishi M, et al. Impact of inferior mesenteric artery lymph node metastasis on the prognosis of left-sided colorectal cancer[J]. Anticancer Res, 2021, 41(5):2533-2542. doi: 10.21873/anticanres.15031 [6] 日本大腸癌研究會. 大腸癌取扱い規約[M]. 9版. 東京: 金原出版株式会社, 2018. [7] Hu SD, Li SY, Teng D, et al. Analysis of risk factors and prognosis of 253 lymph node metastasis in colorectal cancer patients[J]. BMC Surg, 2021, 21(1):280. doi: 10.1186/s12893-021-01276-2 [8] 葛磊,包满都拉,刘正,等.腹腔镜辅助左半结肠切除术中保留与不保留肠系膜下动脉主干的近期疗效比较[J].中华胃肠外科杂志,2020,23(11):1074-1080. doi: 10.3760/cma.j.issn.441530-20191124-00495 [9] 王权,佟伟华,张加鑫.左半结肠癌行No. 223、No. 253淋巴结清扫意义及争议[J].中国实用外科杂志,2020,40(3):284-287. [10] Planellas P, Salvador H, Farrés R, et al. A randomized clinical trial comparing the initial vascular approach to the inferior mesenteric vein versus the inferior mesenteric artery in laparoscopic surgery of rectal cancer and sigmoid colon cancer[J]. Surg Endosc, 2019, 33(4):1310-1318. doi: 10.1007/s00464-018-6551-z [11] Lee KH, Kim JS, Kim JY. Feasibility and oncologic safety of low ligation of inferior mesenteric artery with D3 dissection in cT3N0M0 sigmoid colon cancer[J]. Ann Surg Treat Res, 2018, 94(4):209-215. doi: 10.4174/astr.2018.94.4.209 [12] 梁月祥,梁寒,丁学伟,等.进展期胃癌D2根治术中第14v组淋巴结清扫的意义[J].中华胃肠外科杂志,2013,16(7):632-636. doi: 10.3760/cma.j.issn.1671-0274.2013.07.009 [13] Watanabe J, Ota M, Suwa Y, et al. Evaluation of lymph flow patterns in splenic flexural colon cancers using laparoscopic real-time indocyanine green fluorescence imaging[J]. Int J Colorectal Dis, 2017, 32(2):201-207. doi: 10.1007/s00384-016-2669-4 [14] 赵轩,孙晶.直肠癌和乙状结肠癌根治术中肠系膜下动脉根部淋巴结清扫的相关热点问题及研究进展[J].中国肿瘤外科杂志,2018,10(5):278-282. doi: 10.3969/j.issn.1674-4136.2018.05.002 [15] Li K, Li ZM, Yan BT, et al. Preoperative carbon nanoparticle injection improves inferior mesenteric artery lymph node retrieval in patients with rectal cancer[J]. Surgery, 2022, 171(5):1177-1184. doi: 10.1016/j.surg.2021.08.023 [16] Sun Y, Chi P, Lin H, et al. Inferior mesenteric artery lymph node metastasis in rectal cancer treated with neoadjuvant chemoradiotherapy: incidence, prediction and prognostic impact[J]. Eur J Surg Oncol, 2017, 43(1):85-91. doi: 10.1016/j.ejso.2016.09.005 [17] Rao X, Zhang J, Liu T, et al. Prognostic value of inferior mesenteric artery lymph node metastasis in cancer of the descending colon, sigmoid colon and rectum[J]. Colorectal Dis, 2018, 20(6):O135-O142. doi: 10.1111/codi.14105 [18] Sun YW, Yu D, Zhong JM, et al. Para-aortic lymph node dissection in left-sided colorectal cancer: risk factors, prognostic impact, and therapeutic value[J]. J Surg Oncol, 2022, 125(8):1251-1259. doi: 10.1002/jso.26829 -


 点击查看大图
点击查看大图
图(4) / 表(5)
计量
- 文章访问数: 323
- HTML全文浏览量: 75
- PDF下载量: 32
- 被引次数: 0
