
-
摘要:
目的 利用瘤体外翻于肛门外、直视下量化切除、超低位吻合保肛术, 治疗低位直肠癌, 探讨本术式的可行性。 方法 对97例肿瘤距齿状线2~5cm的低位直肠癌, 实施保肛治疗, 腹部手术遵循全直肠系膜切除原则; 会阴部手术将瘤体外翻于肛门外, 并依据病理分化程度, 直视下量化切除肿瘤, 同时切除直肠系膜“舌部”。术中下切缘送冰冻病理, 进一步指导手术切除范围。对结肠、直肠实施超低位吻合。按量化切除的肿瘤远端肠管切除长度, 将患者分为3组: 1、1.5、≥2cm组, 观察3组局部复发率, 分析吻合口复发与下切缘长度的关系; 计算术中术后下切缘病理无癌残留符合率及直肠系膜“舌部”病理阳性率。按吻合口距齿状线距离不同分为3组: 齿状线组, 0~1 cm组, 1~2 cm组, 对3组肛门节制大便、大便失禁等功能进行评价, 并对患者满意度进行调查。 结果 全组无手术病死率, 并发症发生率5.2%, 局部复发率6.2%, 3年、5年生存率分别为83.3%、72.6%。下切缘长度不同的3组局部复发率分别为2.1%、9.7%、11.1%, 差异无统计学意义.术中术后下切缘病理无癌残留符合率为100%, 直肠系膜“舌部”病理阳性率为1.03%。术后9个月肛门功能优良率评定结果分别为, 齿状线组: 87.0%, 0~1cm组: 97.1%, 1~2 cm组: 100%;术后9个月, 对肛门功能恢复情况进行秩和检验: 各组间P值均 > 0.05, 差异性无统计学意义; 术后6个月无一例大便失禁, 患者满意度均达85%以上。 结论 对于低位直肠癌, 依据病理分化报告结果, 瘤体外翻于肛门外直视下并量化切除后, 在齿状线上2 cm内甚至齿状线处实施超低位吻合的保肛手术简便可行, 效果确切。 Abstract:Objective To investigate the clinical value of quantifiable pull-out resection and ultra-low anastomosis for the treatment of low rectal cancer. Methods Sphincter preserving surgery was performed on 97 patients with low rectal tumors, 2-5 cm away from the dentate line.The operation on the abdominal region was conducted on the basis of the principle of total mesorectal excision. During the operation on the perineum, the tumor was excised from the anus, and macroscopically quantifiable excision was conducted in accordance with the degree of pathological differentiation.Simultaneously, the mesorectal "tongue" was also removed.To determine the scope of the surgical resection, frozen sections of the lower margin of the tumor were prepared during the surgery.An ultra-low anastomosis of the colon and rectum was performed on the patients.On the basis of the length of the quantifiably excised distal intestinal canals, the patients were grouped into three: the 1 cm excision, 1.5 cm excision, and≥2 cm excision groups.The rates of local recurrence in the three groups were observed, and the relationship between the length of resection and recurrence at the intestinal stoma was analyzed.The coincidence rate of cancer-free residuals and the pathological positive rate of the mesorectal "tongue" during and after the surgery were calculated.The patients were divided into three groups using the different spaces from the stoma to the dentate line as bases: the dentate line group, 0-1 cm group, and 1-2 cm group.The functions of the anus in controlling stool and fecal incontinence in these groups were evaluated.Finally, an investigation on the degree of satisfaction of the patients was surveyed. Results No patient died during the surgery in all groups.The incidence of complications was 5.2%and the rate of local recurrence was 6.2%.The 3-and 5-year survival rates were 83.3%and 72.6%, respectively.The recurrence rates of the three groups with different resection lengths were 2.1%, 9.7%, and 11.1%, respectively.No significant differences were observed in the three groups.The coincidence rate of cancer -free residues was 100%, and the pathological positive rate of the mesorectal "tongue" was 1.03%during and after the surgery. Nine months after the surgery, the evaluation results of satisfactory anal functions were as follows: 87.0%in the dentate line group, 97.1%in the 0-1 cm group, and 100.0%in 1-2 cm group.No significant differences were observed in the three groups.Fecal incontinence was not found in these cases at 6 months after surgery, and the rate of satisfaction exceeded 85%in all patients. Conclusion The quantifiable pull-out resection and anastomosis as a mode of anus-preserving surgery is safe and feasible in patients with low rectal cancer. -
Key words:
- Exstrophy of tumor /
- Quantifiable resection /
- Ultra-low rectal cancer
-

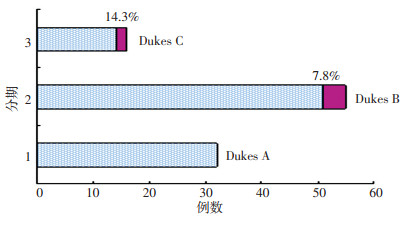
图 1 不同Dukes分期患者局部复发率
Figure 1. Local recurrence rales of patients with different Duke's stages
表 1 患者其他临床资料 /n
Table 1. Clinical characteristics of patients

表 2 局部复发与下切缘的关系 %
Table 2. Relationship between the distal margin of resection and local recurrence

表 3 各组术后肛门功能恢复情况 n
Table 3. Recovery of the anal functions in the three groups

-
[1] 李明. 顾晋. 中国结直肠癌20年来发病模式的变化趋势[J]. 中华胃肠外科杂志, 2004, 3: 214-217. doi: 10.3760/cma.j.issn.1671-0274.2004.03.016 [2] Rengan R, Paty P, Wong WD, et al. Distal cT2N0 rectal cancer: is there an alternative to abdominoperineal resection[J]?J Clin Oncol, 2005, 23(22): 4905-4912. doi: 10.1200/JCO.2005.10.041 [3] 刘宝华, 张胜本, 王亚旭, 等. 肛肠测压在直肠癌术后肛门功能评价中的价值[J]. 第三军医大学学报, 1999, 21(4): 279-281. doi: 10.3321/j.issn:1000-5404.1999.04.015 [4] Cole SP, Bhardwaj G, GerlachJH, et al. Overexpression of a transporter gene in a multidrug-resistant human lung cancer cell line. Science, 1992, 258(5088): 1650-1654. [5] Nelson H, Petrelli N, Carlin A, et al. Guidelines 2000 for colon and rectal cancer surgery[J]. J Natl Cancer Inst. 2001, 93(8): 583 -596. [6] Andreola S, Leo E, Belli F, et al. Distal intramural spread in adeno⁃ carcinoma of the lower third of the rectum treated with total rectal resection and coloanal anastomosis[J]. Dis Colon Rectum, 1997, 40 (1): 25-29. [7] 董新舒, 李志高, 徐海涛. 从术后局部复发形式探讨低位直肠癌保肛手术适应症[J]. 中国实用外科杂志, 2005, 25(3): 131-132. doi: 10.3321/j.issn:1005-2208.2005.03.002 [8] 郁宝铭. 保肛手术在直肠癌中的地位[J]. 国际外科学杂志. 2007, 34 (11): 724-727. doi: 10.3760/cma.j.issn.1673-4203.2007.11.002 [9] 张文范. 消化系统癌症手术与综合治疗. 第1版[M]. 辽宁: 辽宁科学技术出版社, 1999, 390-391. [10] Kwok SP, Lau WY, Leung KL, et al. Prospective analysis of the distal margin of clearance in anterior resection for rectal carcinoma[J]. Br J Surg, 1996, 83(7): 969-972. [11] 孙学军, 吕春华, 黄凤瑞, 等. 低位直肠癌行保留内括约肌管扎式结肠肛管吻合术的效果[J]. 实用医药杂志, 2007, 24(7): 775-778. doi: 10.3969/j.issn.1671-4008.2007.07.003 [12] 张红岩, 田景中. TME和DST在低位直肠癌保肛手术中的应用[J]. 浙江临床医学, 2007, 9(10): 1340. doi: 10.3969/j.issn.1008-7664.2007.10.029 [13] Piso P, Dahlke MH, Mirena P, et al. Total mesorectal excision for middle and lower rectal cancer: a single institution experience with 337 consecutive patients[J]. J Surg Oncol, 2004, 86(3): 115-121. doi: 10.1002/jso.20062 [14] Heald RJ, Karanjia ND. Results of radical surgery for rectal cancer[J]. World J Surg, 1992, 16(5): 848-857. doi: 10.1007/BF02066981 [15] Piso P, Dahlke M, Mierna P, et al. Total mesorectal excision for middle and lowe rerctal cancer: a singl ei nstitution experience with337 consecutive patients[J]. J Surg Oncol, 2004, 86(3): 115-121. doi: 10.1002/jso.20062 -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 52
- HTML全文浏览量: 6
- PDF下载量: 0
- 被引次数: 0
