
Case-matched Analysis of Total Laparoscopic Anatomic versus Open Hepatectomy for Hepatocellular Carcinoma in the Left Lobe
-
摘要:
目的 探讨完全腹腔镜解剖性肝切除治疗左叶肝细胞癌的可行性及其疗效。 方法 自2006年6月至2009年12月间, 总结南昌大学第二附属医院肝胆外科收治21例确诊为左叶肝细胞癌且已行完全腹腔镜解剖性肝切除(laparoscopic anatomic hepateetomy, LAH)患者的围手术期的临床资料, 构成LAH研究组。在同一时间段, 以患者年龄、手术方式、肿瘤大小、肝硬化程度为配对条件, 在开腹解剖性肝切除治疗左叶肝细胞癌的病例库中进行1:1配对抽选, 共21例纳入LAH配对组。 结果 LAH研究组的手术时间为(156.67±32.15)min, 术中失血量为(157.14±40.51)mL, 两者均少于配对组(P=0.036, P < 0.001)。LAH研究组术后患者平均镇痛剂使用时间为(2.19±0.51)d, 平均首次进食时间为(2.24±0.44)d, 平均首次离床活动时间为(2.71±0.78)d, 平均住院时间为(7.86±1.24)d, 均优于配对组(P < 0.05)。两组并发症及死亡率差异没有统计学意义。术后中位随访期为21个月, LAH研究组的1、3年总体生存率分别为86%、62%, 配对组的1、3年总体生存率分别为90%、67%, Log-rank比较两组肝癌患者生存曲线差异无统计学意义。 结论 完全腹腔镜解剖性肝切除术治疗左叶肝细胞癌是安全可行, 具有一定的近期优势, 且术后总体生存率与开腹肝切除术相比无差别。 Abstract:Objective To evaluate the surgical results and mid-term survival of the cases undergoing total laparoscopic anatomic hepatectomy(LAH) for hepatocellular carcinoma(HCC) in the left lobe. Methods From June 2006 to December 2009, clinical records of 21 patients with HCC in the left lobe who underwent a total LAH operation were included in the LAH study group.During the same period, data on the matched-pair group of another 21 patients who underwent open anatomic hepatectomy were included in the LAH matched-pair group.The two groups were compared in terms of age, type of resection, tumor size, and severity of liver cirrhosis. Results The laparoscopic approach resulted in shorter duration of surgery(156.67±32.15 min, P=0.036) and less blood loss(157.14±40.51 mL, P=0.000) in the LAH study group, compared to the LAH matched-pair group.Statistically significant differences were found in the primary-porta-hepatic surgery duration between the LAH study group and the matched-pair group(P=0.001).The mean duration of the secondary-porta-hepatic surgery was similar for the two groups(P=0.061).In the LAH study group, the mean time for required analgesic medication(2.19±0.51 d vs.3.10±1.04 d), food intake(2.24±0.44 d vs.3.81±0.40 d), first ambulation time(2.71±0.78 d vs.3.52±0.93 d), and average stay (7.86±1.24 d vs.10.95±1.40 d) were all better than those of the matched-pair group(P < 0.05).No statistical significance in the perioperative morbidity and mortality rate were found between the two groups.After a median follow up of 21 months, the 1 and 3-year overall survival rates after liver excision for HCC were 86%and 62%in LAH study group, respectively, and those in the matched-pair group were 90%and 67%, respectively.No significant differences were observed in the survival curves in the present study. Conclusion The total LAH of HCC in the left lobe is feasible and safe for the selected patients and may result in good surgical results, with similar benefits in the overall survival. -
Key words:
- Laparoscopy /
- Liver neoplasm /
- Hepatocellular carcinoma /
- Hepatectomy
-

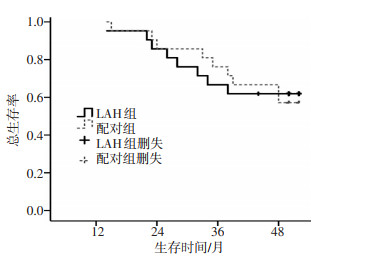
图 1 LAH研究组与配对组肝细胞癌患者的总体生存曲线
Figure 1. Overall survival rates in LAH study group and LAH matched-pair group of patients with hepatocellular carcinoma
表 1 LAH研究组与配对组的均衡性检验 n %
Table 1. Comparison of demographic and clinical data between the two groups

表 2 LAH研究组与配对组的手术情况 n %
Table 2. Surgical details of patients in LAH study group and LAH matched-pair group

表 3 LAH研究组与配对组的术后恢复及并发症情况
Table 3. Postoperative parameters and complications in LAH study group and LAH matched-pair group

-
[1] 王磊. 腹腔镜肝切除术的发展现状[J]. 腹腔镜外科杂志, 2011, 16(3): 167-168. https://www.cnki.com.cn/Article/CJFDTOTAL-FQJW201609019.htm [2] Nguyen KT, Gamblin TC, Geller DA. World review of laparoscopic liver resection-2, 804 patients[J]. Ann Surg, 2009, 250(5): 831-841. doi: 10.1097/SLA.0b013e3181b0c4df [3] 刘荣, 黄志强, 周宁新, 等腹腔镜解剖性旰切除技术研究[J]. 肝胆外科杂志, 2005, 13(2): 96-98. doi: 10.3969/j.issn.1006-4761.2005.02.006 [4] 蔡秀军, 王一帆. 腹腔镜肝切除术中出血的控制[J]. 中华外科杂志, 2010, 48(3): 171-172. doi: 10.3760/cma.j.issn.0529-5815.2010.03.005 [5] Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey[J]. Ann Surg, 2004, 240(2): 205-213. doi: 10.1097/01.sla.0000133083.54934.ae [6] Kazaryan AM, Pavlik Marangos I, Rosseland AR, et al. Laparoscopic liver resection for malignant and benign lesions: ten-year Norwegian single-center experience[J]. Arch Surg, 2010, 145(1): 34-40. http://archsurg.jamanetwork.com/data/Journals/SURG/5378/soa90021_34_40.pdf [7] 蔡秀军, 郑雪咏. 腹腔镜肝脏切除需关注的一些问师[J]. 中华医学杂志, 2010, 90(24): 1657-1659. doi: 10.3760/cma.j.issn.0376-2491.2010.24.001 [8] 张志波, 郑树国, 李建伟, 等. 腹腔镜肝切除术治疗肝细胞癌37例临床分析[J]. 中华普通外科杂志, 2009, 24(10): 806-808. doi: 10.3760/cma.j.issn.1007-631X.2009.10.009 [9] 刘荣. 腹腔镜解剖性肝切除的理念与实践[J]. 中华外科杂志, 2008, 46(23): 1766-1767. doi: 10.3321/j.issn:0529-5815.2008.23.003 [10] 李晓平, 周杰, 徐达传, 等. 第一肝门的腹腔镜肝脏手术入路解剖学研究[J]. 中国临床解剖学杂志, 2004, 22(3): 230-233. doi: 10.3969/j.issn.1001-165X.2004.03.002 [11] Aldrighetti L, Guzzetri E, Pulitano C, et al. Case-matched analysb of totally laparoscopic versus open liver resection for HCC: short and middle term results[J]. J Surg Oncol, 2010, 102(1): 82-86. doi: 10.1002/jso.21541 -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 15
- HTML全文浏览量: 30
- PDF下载量: 0
- 被引次数: 0
