
Clinical Observation of Primary Central Nervous System Lymphoma Patients with Treatment of Temozolomide-based Chemotherapy and Radiation Therapy Treatments
-
摘要:
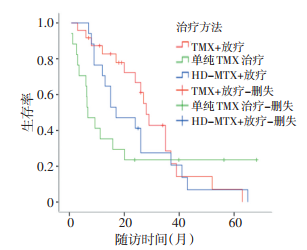
目的 评价以替莫唑胺为主的化疗联合放疗治疗原发中枢神经系统淋巴瘤(PCNSL)的疗效及不良反应。 方法 对2006年6月至2012年3月山东省肿瘤医院收治的24例PCNSL患者采用全脑放疗同步替莫唑胺化疗之后, 给予替莫唑胺+奈达铂+长春新碱化疗方案行6~8个周期的辅助化疗。观察患者肿瘤缓解状态、总生存期及不良反应。 结果 24例均完成治疗。随访3~63个月, 中位生存时间为25个月, 治疗后CR者41.7%(10/24), PR者29.2%(7/24), SD者12.5%(3/24), PD者16.7%(4/24), 客观肿瘤缓解率(ORR)为70.8%。Kaplan-Meier分析显示该治疗方案优于大剂量甲氨蝶呤(HD-MTX)联合放疗治疗PCNSL的效果, 亦优于单药替莫唑胺治疗PCNSL的效果, 且不良反应小。 结论 替莫唑胺为主的化疗联合放疗治疗PCNSL较安全、效果好。 -
关键词:
- 原发性中枢神经系统淋巴瘤 /
- 替莫唑胺 /
- 放射疗法 /
- 药物疗法
Abstract:Objective To evaluate the therapeutic efficacy and toxicity of novel temozolomide-based chemotherapy regimen with radiotherapy for treating primary central nervous system lymphoma (PCNSL). Methods Twenty-four patients were treated by concurrent chemoradiation with temozolomide, after which adjuvant chemotherapy (temozolomide, nedaplatin, and vincristine) was given for 6-8 cycles. Some states were observed, including remission rate, overall survival (OS), and toxicity. Results The 24 patients were followed up for 3 months to 63 months. The median overall survival was 25 months. Ten patients (41.7%) achieved complete response (CR), whereas seven patients (29.2%) achieved partial response (PR). Stable disease was documented in three patients (12.5%), whereas progressive disease occurred in four patients (16.7%). The objective response rate (ORR) was 70.8%. Kaplan-Meier analysis shows that the new treatment is better and results in less adverse reactions than does the combination of high-dose methotrexae (HD-MTX) and radiotherapy, and superior to the single-agent temozolomide treatment of PCNSL. Conclusion The temozolomide-based chemo- therapy regimen with radiotherapy for PCNSL treatment is safe and effective. -
Key words:
- Primary central nervous system lymphoma /
- Temozolomide /
- Radiotherapy /
- Chemotherapy
-

图 1 本组与国内外同期研究的患者生存曲线比较
Figure 1. Comparison of survival curves in patients of grouping the present study and in studies at home and abroad over the same period
表 1 24例PCNSL患者的临床特征
Table 1. The clinical features of 24 patients with PCNSL

-
[1] Villano JL, Koshy M, Shaikh H, et al. Age, gender, and racial differences in incidence and survival in primary CNS lymphoma[J]. Br J Cancer, 2011, 105(9): 1414-1418. doi: 10.1038/bjc.2011.357 [2] Ferreri AJ, Marturano E. Primary CNS lymphoma[J]. Best Pract Res Clin Haematol, 2012, 25(1): 119-130. doi: 10.1016/j.beha.2011.12.001 [3] Gerard LM, Imrie KR, Mangel J, et al. High-dose methotrexate based chemotherapy with deferred radiation for treatment of newly diagnosed primary central nervous system lymphoma. Leuk Lymphoma[J]. Leuk Lymphoma, 2011, 52(10): 1882-1890. doi: 10.3109/10428194.2011.584004 [4] Küker W, Nägele T, Thiel E, et al. Primary central nervous system lymphomas (PCNSL): MRI response criteria revised[J]. Neurology, 2005, 65(7): 1129-1131. doi: 10.1212/01.wnl.0000178894.51436.54 [5] 郑伟, 聂青, 康静波, 等. 原发中枢神经系统淋巴瘤17例临床分析[J]. 中国肿瘤临床, 2009, 36(10): 554-558. doi: 10.3969/j.issn.1000-8179.2009.10.005 [6] Makino K, Nakamura H, Hide T, et al. Salvage treatment with temozolomide in refractory or relapsed primary central nervous system lymphoma and assessment of the MGMT status[J]. J Neurooncol, 2012, 106(1): 155-160. doi: 10.1007/s11060-011-0652-z [7] DeAngelis LM, Seiferheld W, Schold SC, et al. Combination chemotherapy and radiotherapy for primary central nervous system lymphoma: Radiation Therapy Oncology Group Study 93-10[J]. J Clin Oncol, 2002, 20(24): 4643-4648. doi: 10.1200/JCO.2002.11.013 [8] Omuro AM, Ben-Porat LS, Panageas KS, et al. Delayed neurotoxicity in primary central nervous system lymphoma[J]. Arch Neurol, 2005, 62(10): 1595-1600. [9] Poortmans PM, Nelemans HC, Reiche H, et al. High-dose methotrexate-based chemotherapy central nervous system lymphoma: European Organization for Research and Treatment of Cancer Lymphoma Group Phase Ⅱ Trial 20962[J]. J Clin Oncol, 2003, 21(24): 4483-4488. doi: 10.1200/JCO.2003.03.108 [10] 潘浩. 新型烷化剂替莫唑胺的临床应用进展[J]. 中国医院用药评价与分析, 2010, 10(6): 489-490. https://www.cnki.com.cn/Article/CJFDTOTAL-YYPF201006007.htm [11] Reni M, Zaja F, Mason W, et al. Temozolomide as salvage treatment in primary brain lymphomas[J]. Br J Cancer, 2007, 96(6): 864-867. doi: 10.1038/sj.bjc.6603660 [12] Christmann M, Verbeek B, Roos WP, et al. O(6)-Methylguanine-DNA methyltransferase (MGMT) in normal tissues and tumors: Enzyme activity, promoter methylation and immunohistochemistry[J]. Biochim Biophys Acta, 2011, 1816(2): 179-190. [13] 陈忠平, 杨群英. 神经系统肿瘤化疗手册[M]. 北京: 北京大学医学出版社, 2012: 36-37. [14] Ferreri AJ, Licata G, Foppoli M, et al. Clinical relevance of the dose of cytarabine in the upfront treatment of primary CNS lymphomas with methotrexate-cytarabine combination[J]. Oncologist, 2011, 16(3): 336-341. doi: 10.1634/theoncologist.2010-0361 [15] Fritsch K, Kasenda B, Hader C, et al. Immunochemotherapy with rituximab, methotrexate, procarbazine, and lomustine for primary CNS lymphoma (PCNSL) in the elderly[J]. Ann Oncol, 2011, 22(9): 2080-2085. doi: 10.1093/annonc/mdq712 -

 下载:
下载:
 点击查看大图
点击查看大图
图(1) / 表(1)
计量
- 文章访问数: 21
- HTML全文浏览量: 2
- PDF下载量: 1
- 被引次数: 0
