
-
摘要:
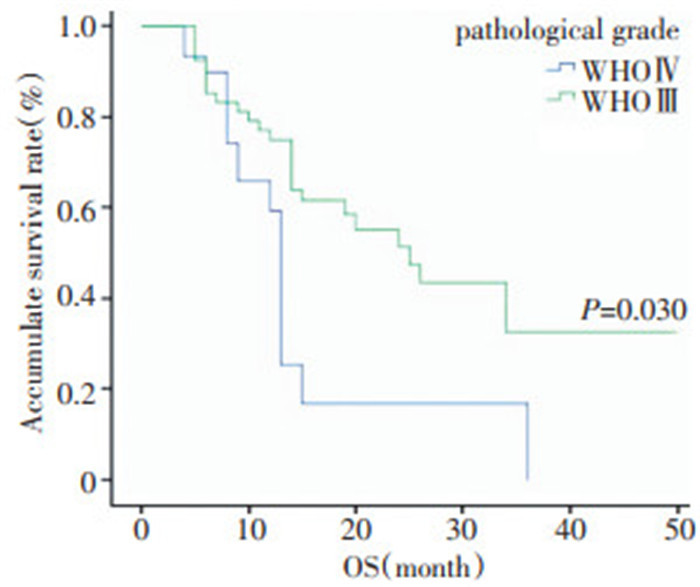
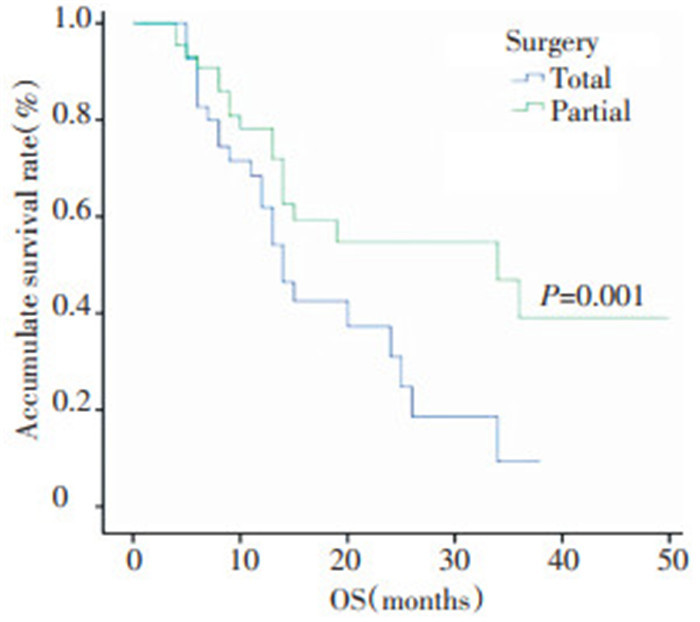
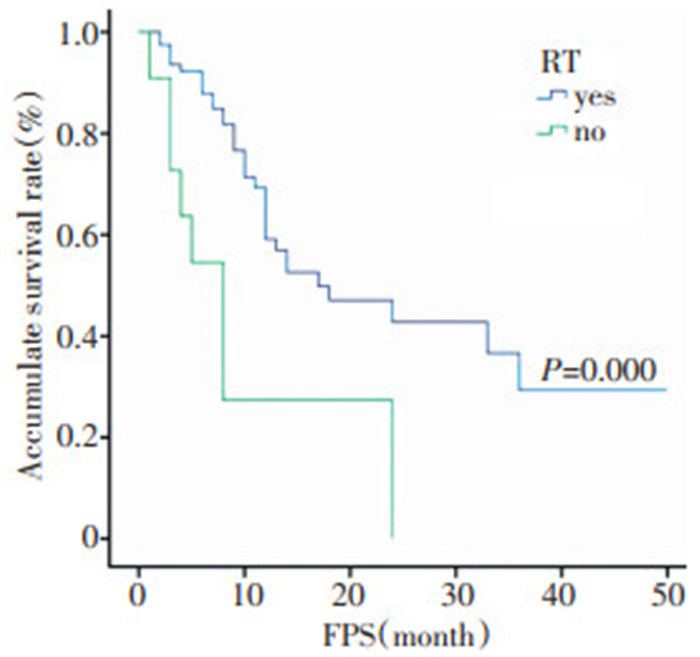
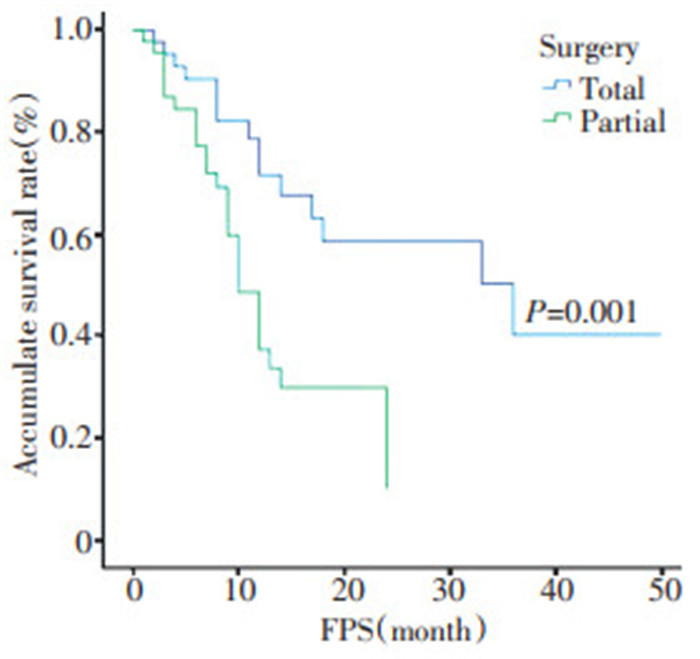
目的 探讨高度恶性脑胶质瘤的预后以及预后影响因素。 方法 回顾分析江西省肿瘤医院2005年4月至2011年2月收治的89例高度恶性脑胶质瘤的临床资料, 其中手术全切43例, 部分切除46例; WHO3级45例, 4级44例。 结果 全组中位生存期13个月, 2年总生存率(OS)及无进展生存率(PFS)分别为43.2%和36.9%;单因素分析显示切除程度、病理分级、年龄是OS的影响因素(P < 0.05), 切除程度、脑室系统受侵、术后放疗是PFS的影响因素(P < 0.05), 多因素分析结果显示切除程度、年龄是OS的独立影响因素(P < 0.05);切除程度、术后放疗是PFS的独立影响因素(P < 0.05);全组共41例复发, 其中原位复发65.9%, 远隔部位复发34.1%;46例脑室系统受侵者, 11例出现远隔部位复发; 其余43例, 仅3例出现远隔部位复发。 结论 手术切除程度、年龄是影响OS的独立预后因素, 术后放疗能改善PFS; 原位复发是主要复发模式, 脑室受侵增加了远处播散概率。 Abstract:Objective This study discusses the prognosis and prognostic factors of postoperative high-grade glioma. Methods Eighty-nine patients with postoperative high-grade glioma were registered at the Jiangxi Province Tumor Hospital between April 2005 and February 2011.Total and partial removal of glioma were performed in 43 and 46 patients, respectively.Based on the World Health Organization(WHO) grading system of glioma, 45 patients in this study had WHO gradeⅢglioma and 44 patients had WHO grade IV glioma. Results The results show that the median survival time of patients with glioma was 13 months.The two-year overall survival rate(OS) was 43.2%, and the two-year progression-free survival rate(PFS) was 36.9%.The prognostic factors of OS identified in univariate analysis include age, pathological grade, and resection extent(P < 0.05).However, the independent prognostic factors in multivariate analysis only include resection extent and age(P < 0.05).The prognostic factors of PFS in univariate analysis include resection extent, postoperative radiotherapy, and ventricle violated before surgery(P < 0.05).However, the independent prognostic factors in multivariate analysis only include resection extent and postoperative radiotherapy(P < 0.05).In this study, tumor recurrence occurred in 41 patients, 65.9% patients had tumor bed failure, and 34.1% had distance failure.Among the 46 patients with damaged ventricles before surgery, 11 displayed distant recurrence.Among the 43 patients who underwent total removal of glioma, 3 had distant metastasis before surgery Conclusion Resection extent and age are the independent prognostic factors of overall survival in glioma, and postoperative radiotherapy can improve the progression-free survival of patients.The major pattern of failure is tumor bed recurrence.However, distance failure increases when the ventricle is damaged. -
Key words:
- high-grade glioma /
- prognosis /
- patterns of failure
-

图 1 不同年龄组的总生存曲线比较
Figure 1. Overall survival curves in patients of different age groups

图 2 不同病理分级的总生存曲线比较
Figure 2. Overall survival curves in patients with various pathological grades

图 3 不同手术切除程度的总生存曲线比较
Figure 3. Overall survival curves in patients with resection of different extent

图 4 术后是否放疗的无进展生存曲线比较
Figure 4. Progression-free survival curves in patients with or without radiotherapy after surgery

图 5 不同手术切除程度的无进展生存曲线比较
Figure 5. Progression-free survival curves in patients with resection of different extent

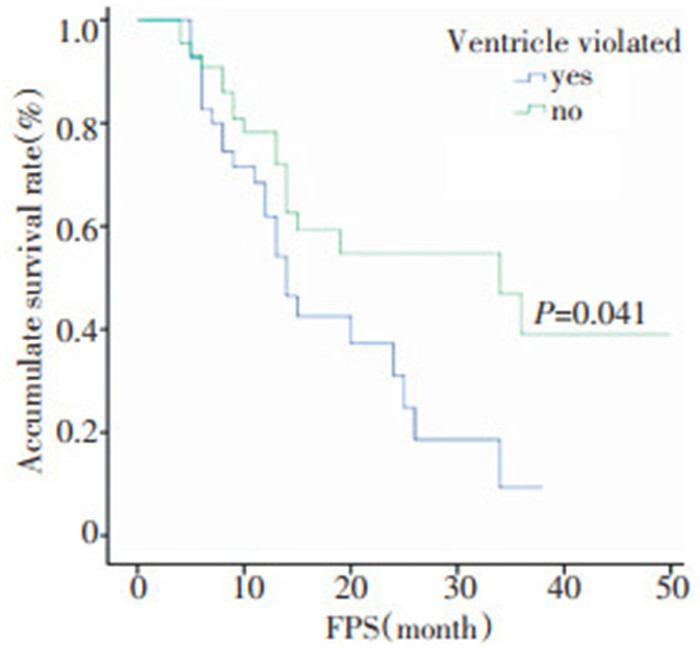
图 6 脑室系统是否受侵的无进展生存曲线比较
Figure 6. Progression-free survival curves in patients with or without ventriclular violation
表 1 影响OS的多因素分析
Table 1. Multivariate analysis of prognostic factors for OS rates in 89 high grade glioma patients

表 2 影响PFS的多因素分析
Table 2. Multivariate analysis of prognostic factors for PFS rates in 89 high grade glioma patients

表 3 影响OS及PFS的单因素分析
Table 3. Univariate analysis of prognostic factors affecting OS and PFS rates in 89 high grade glioma patients

表 4 脑室系统是否受侵与复发部位关系 例
Table 4. Relationship between the location of tumor recurrence and damaged ventricle(n)

-
[1] 汪洋, 盛晓芳, 高晶, 等. 高分级神经胶质瘤112例术后放、化疗疗效及其预后分析[J]. 肿瘤, 2009, 29(7): 688-672. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLL200907020.htm [2] Duncan GG, Goodman GB, Ludgate CM, et al. The treatment ofadult supratentorial high grade astrocytomas[J]. J Neuro Oncol, 1992, 13(1): 63-72. [3] atalán-Uribarrena G, Bilbao-Barandica G, Pomposo-Gaztelu I, etal. Prognostic factors and survival in a prospective cohort of pa tients with high-grade glioma treated with carmustine wafers or te mozolomide on an intention-to-treat basis[J]. Acta Neurochir, 2012, 154(2): 211-222. doi: 10.1007/s00701-011-1199-7 [4] Irwin C, Hunn M, Purdie G, et al. Delay in radiotherapy shortenssurvival in patients with high grade glioma[J]. J Neuro Oncol, 2007, 85(3): 339-343. doi: 10.1007/s11060-007-9426-z [5] Mohamed A, Ahmed E. Hypofractionated conformal irradiation ofpatients with malignant glioma[J]. J Egypt Natl Cancer Insti, 2012, 24: 139-143. doi: 10.1016/j.jnci.2012.07.001 [6] Dea N, Fournier-Gosselin MP, Mathieu D, et al. Does extent of re section impact survival in patients bearing glioblastoma[J]. Can JNeurol Sci, 2012, 39(5): 632-637. doi: 10.1017/S0317167100015377 [7] Uehara K, Sasayama T, Miyawaki D, et al. Patterns of failure aftermultimodal treatments for high-grade glioma: effectiveness ofMIB-1 labeling index[J]. Radiat Oncol, 2012, 26(7): 104-115. [8] Yamaguchi S, Kobayashi H, Terasaka S, et al. The impact of extentof resection and histological subtype on the outcome of adult pa tients with high-grade gliomas[J]. Jpn J Clin Oncol, 2012, 42(4): 270-277. doi: 10.1093/jjco/hys016 [9] 邹燕梅, 熊华, 于世英. 恶性胶质瘤术后治疗疗效及预后因素分析[J]. 实用癌症杂志, 2009, 24(2): 184-187. doi: 10.3969/j.issn.1001-5930.2009.02.023 [10] Izmalov TR, Pan'shin GA, Datsenko PV. The role of age and tu mor grade in the choice of fractionation regimen in patients with high-grade gliomas[J]. Vopr Onkol, 2012, 58(3): 374-379. [11] Lee SW, Fraass BA, Marsh LH, et al. Patterns of failure following high-dose 3-D conformal radiotherapy for high-grade astrocyto mas: a quantitative dosimetric study[J]. Int J Radiat Oncol BiolPhys, 1999, 43(1): 79-88. doi: 10.1016/S0360-3016(98)00266-1 [12] Chan JL, Lee SW, Fraass BA, et al. Survival and failure patterns of high-grade gliomas after three-dimensional conformal radiothera py[J]. J Clin Oncol, 2002, 20(6): 1635-1642. doi: 10.1200/JCO.2002.20.6.1635 [13] Wei T, Denice D, Jia H, et al. Conditional survival of high-gradeglioma in Los Angeles County during the year 1990-2000[J]. J Neu ro Oncol, 2012, 110(1): 145-152. doi: 10.1007/s11060-012-0949-6 [14] 顾文栋, 裴红蕾. 69例脑胶质瘤术后三维适形放射治疗临床分析[J]. 中国神经肿瘤杂志, 2011, 9(2): 124-127. [15] Hess CF, Schaaf JC, Kortmann RD, et al. Malignant glioma: pat terns of failure following individually tailored limited volume irradi ation[J]. Radiother Oncol, 1994, 30(2): 146-149. doi: 10.1016/0167-8140(94)90044-2 -

 下载:
下载:
 点击查看大图
点击查看大图

计量
- 文章访问数: 8
- HTML全文浏览量: 0
- PDF下载量: 0
- 被引次数: 0
