
Magnetic resonance imaging outcome of residual tumor after ultrasound ablation for uterine fibroids
-
摘要:
目的 研究超声消融子宫肌瘤后残余瘤组织的核磁共振成像(MRI)转归。 方法 对重庆医科大学附属第一医院74例子宫肌瘤患者(77个肌瘤)进行超声消融治疗。根据超声消融后1个月内所测体积消融率(消融率), 将74例患者分为三组。A组(24例): 消融率 > 90%;B组(28例): 消融率70%~90%;C组(22例): 消融率 < 70%。MRI监测三组治疗后1、3、6、12个月残余瘤组织的体积变化, 随访超声消融治疗后靶肌瘤的再治疗情况。 结果 1) 治疗后1、3、6、12个月所测残余瘤组织平均体积, 消融率 > 90%组分别为(3.18±1.70)cm3、(1.88±0.99)cm3、(1.00±0.54)cm3、(0.44±0.20)cm3, 呈明显缩小趋势(P < 0.01)。消融率70%~90%组为(6.72±3.06)cm3、(7.41±4.67)cm3、(5.19±3.91)cm3、(4.75±3.17)cm3, 呈现缩小趋势(P < 0.05)。消融率 < 70%组为(17.95±8.85)cm3, (22.10±13.30)cm3、(23.31±13.37)cm3、(23.93±12.85)cm3, 体积变化差异无显著性统计学意义(P > 0.05)。2)治疗后12个月再次治疗情况: 消融率 > 90%者, 无一例在治疗后12个月内需要再次干预治疗, 消融率70%~90%者及消融率 < 70%者分别有10.7%及54.5%患者在治疗后12个月内再次行超声消融或手术治疗。 结论 超声消融率≥70%组的残余瘤组织的体积在术后12个月内呈明显缩小转归趋势, 并且治疗后靶肌瘤的再干预情况明显少于消融率 < 70%组。消融的体积越大, 再治疗的机会越小。 Abstract:Objective This study aimed to determine the outcome of the residual tissue measured by magnetic resonance imaging(MRI) after ultrasound ablation for uterine fibroids. Methods A total of 77 patients with uterine fibroids subjected to high-intensity focused ultrasound ablation were enrolled in this study undertaken in the First Affiliated Hospital of the Chongqing Medical University.The patients were grouped into three based on the different non-perfused volume(NPV) rates measured by MRI within 1 month after ultrasound ablation.Group A comprised 24 patients whose NPV ratios were more than 90%.Group B comprised 28 patients whose NPV ratios were from 70% to 90%.Group C comprised 22 patients whose NPV ratios were less than 70%.MRI was used to monitor the change in residual tumor volume of the three groups 1, 3, 6, and 12 months after treatment.All re-treated cases were recorded. Results The mean residual tumor volumes of group A were 3.18 ± 1.70, 1.88 ± 0.99, 1.00 ± 0.54, 0.44 ± 0.20 cm3at 1, 3, 6, and 12 months after treatment, respectively.These results indicated a significant decrease with time(P < 0.01).The mean residual tumor volumes of group B were 6.72 ± 3.06, 7.41 ± 4.67, 5.19 ± 3.91, 4.75 ± 3.17 cm3 at 1, 3, 6, and 12 months after treatment, respectively.These results indicated a decrease with time(P < 0.05).The mean residual tumor volumes of group C were 17.95 ± 8.85, 22.10 ± 13.30, 23.31 ± 13.37, 23.93 ± 12.85 cm3 at 1, 3, 6, and 12 months after treatment, respectively.No significant change was found(P > 0.05).No case in group A required re-intervention.The re-intervention rates in groups B and C were 10.7% and 54.5%, respectively, within 12 months after treatment. Conclusion In cases where the ablation rate was equal to or more than 70%, the volume of residual tumor significantly decreased within 12 months after treatment, and the re-intervention rate was less than cases of less than 70%.Fewer incidences of re-treatment resulted in a higher ablation rates. -
Key words:
- ultrasound ablation /
- uterine fibroid /
- residual tumor /
- magnetic resonance imaging /
- outcome
-

图 1 Hifu_3DTPS软件重建及测量子宫肌瘤体积
Figure 1. Hifu_3DTPS software reconstruction and measurement of theuterine fibroid volume
A: MRI(T2 Weighted)measurement of the uterine fibroid volume; B: 3D software reconstruction of targeted area of uterine fibroid

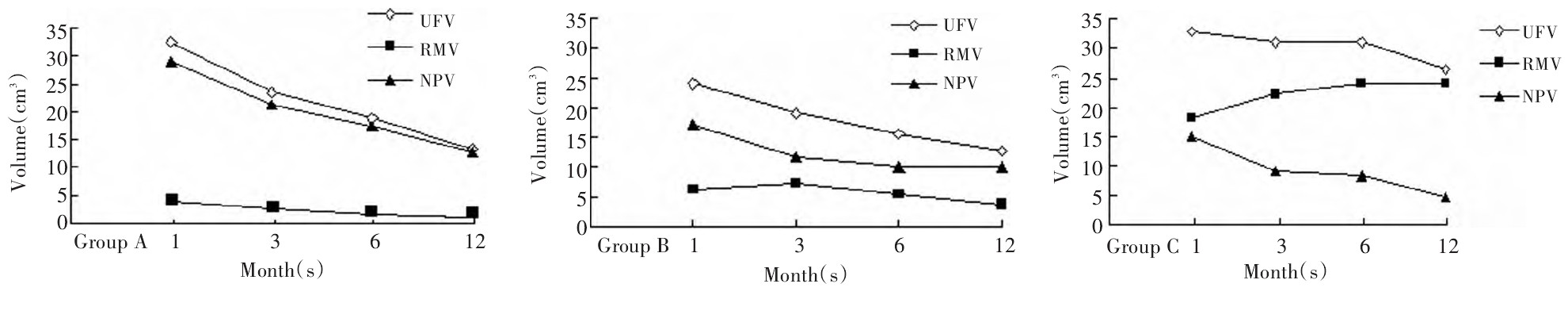
图 2 超声消融治疗后A、B、C三组靶肌瘤体积(UFV)、残余瘤组织体积(RMV)及无灌注区体积(NPV)治疗后1、3、6、12个月的变化(cm3体积)
Figure 2. Change in UFV, RMV and NPV in the three treatment groups 1, 3, 6 and 12 months after HIFU(cm3Volume)
表 1 三组患者的基本情况
Table 1. General characteristics of patients in the three treatment groups

表 2 子宫肌瘤及残余瘤组织体积转归
Table 2. Prognosis of uterine fibroid and residual tumor volume

表 3 三组患者再治疗情况
Table 3. Re-treatment cases in the three treatment groups

-
[1] Zhang L, Chen WZ, Liu YJ, et al. Feasibility of magnetic resonanceimaging-guided high intensity focused ultrasound therapy for ablatinguterine fibroids in patients with bowel lies anterior to uterus[J]. Eur JRadiol, 2010, 73(2): 396-403. [2] 陈文直, 唐良萏, 杨武威, 等. 超声消融治疗子宫肌瘤的安全性及有效性[J]. 中华妇产科杂, 2010, 45(12): 909-912. https://cdmd.cnki.com.cn/Article/CDMD-10631-1016007273.htm [3] 朱丽, 陈文直, 陈锦云, 等. 子宫肌瘤超声消融与MRI信号特征关系的研究[J]. 第三军医大学学报, 2009, 31(14): 1370-1373. doi: 10.3321/j.issn:1000-5404.2009.14.012 [4] 高强度聚焦超声肿瘤治疗系统临床应用指南(试行)[J]. 中华医学杂志, 2005, 85: 796-797. [5] 乐杰, 主编. 妇产科学[M]. 第7版. 北京: 人民卫生出版社, 2008: 6. [6] 史常旭, 辛晓燕, 主编. 现代妇产科治疗学[M]. 第3版. 北京: 人民军医出版社, 2010: 160-168. [7] Hanafi M. Predictors of leiomyoma recurrence after myomectomy[J]. Obstet Gynecol, 2005, 105(4): 877-881. doi: 10.1097/01.AOG.0000156298.74317.62 [8] Kroencke TJ, Scheurig C, Poellinger A, et al. Uterine artery embolization for leiomyomas: percentage of infarction predicts clinical outcome[J]. Radiology, 2010, 255(3): 834-841. doi: 10.1148/radiol.10090977 [9] Holub Z, Eim J, Jabor A, Hendl A. Complications and myoma recurrence after laparoscopic uterine artery occlusion for symptomatic myomas[J]. J Obstet Gynaecol Res. 2006, 32(1): 55-62. [10] Stewart EA, Gostout B, Rabinovici J, et al. Sustained relief of leiomyoma symptoms by using focused ultrasound surgery[J]. Obstet Gynecol, 2007, 110: 279-287. doi: 10.1097/01.AOG.0000275283.39475.f6 [11] Fennessy FM, Tempany CM, Mc Dannold NJ, et al. Uterine leiomyomas: MR imaging-guided focused ultrasound surgery-results ofdifferent treatment protocols[J]. Radiology, 2007, 243(3): 885-893. doi: 10.1148/radiol.2433060267 [12] Hindley J, Gedroyc WM, Regan L, et al. MRI guidance of focusedultrasound therapy of uterine fibroids: early results[J]. AJR Am JRoentgenol, 2004, 183(6): 1713-1719. doi: 10.2214/ajr.183.6.01831713 [13] J. Rabinovici, Y. Inbas, A. Revel. Clinical improvement and shrinkage of uterine fibroids after thermal ablation by magnetic resonance-guided focused ultrasound surgery[J]. Ultrasound ObstetGynecol, 2007, 30: 771-777. [14] Walocha JA, Litwin JA, Miodoński AJ. Vascular system of intramural leiomyomata revealed by corrosion casting and scanning electron microscopy[J]. Hum Reprod, 2003, 18(5): 1088-1093. doi: 10.1093/humrep/deg213 -

 下载:
下载:
 点击查看大图
点击查看大图

计量
- 文章访问数: 42
- HTML全文浏览量: 2
- PDF下载量: 1
- 被引次数: 0
