
-
摘要:
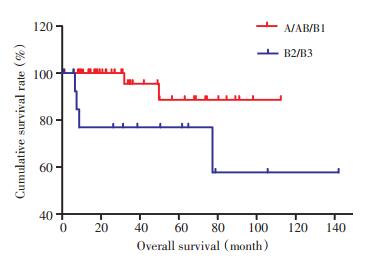
目的 总结单一医生组原发性纵隔肿瘤外科治疗的长期随访。 方法 数据来自北京大学肿瘤医院2000年1月至2014年1月的前瞻性数据库。分析纵隔肿瘤数据库中以根治切除为目的患者的远期生存。 结果 本组常见肿瘤依次为胸腺上皮肿瘤95例(50%),神经源性肿瘤26例(13.7%),纵隔生殖细胞肿瘤26例(13.7%)。全组患者行R0切除者179例(94.2%),R2切除者8例(4.2%),单纯探查者3例(1.6%),术后30d内死亡2例。胸腺上皮肿瘤1、3和5年生存率分别为95%、92.7%和85.7%。根据Masaoka-Koga分期,Ⅰ、Ⅱ、Ⅲ和Ⅳ期胸腺上皮肿瘤的5年生存率分别为100%、82.1%、90%和37.5%。多因素分析显示Masaoka-Koga分期是胸腺上皮肿瘤手术后独立预后因素。A+AB+B1型与B2+B3型胸腺瘤5年生存率分别为88.6%与76.9%,差异具有统计学意义(P < 0.05)。神经源性纵隔肿瘤多为良性,完整切除后均长期生存。 结论 纵隔肿瘤组织学复杂,根据其来源、性质、部位及大小来决定治疗。虽然本组患者生存良好,但单一医生组很难做到前瞻性,大样本研究。因此,对纵隔肿瘤尤其是胸腺上皮肿瘤亟需大样本,多中心合作的前瞻性研究,以找到合理的治疗方式。 Abstract:Objective Mediastinal tumors are tumors derived from different organs. Due to its rarity, few clinical consensuses on its diagnosis and treatments have been concluded. This paper aims to summarize the experiences of a single-surgeon team on the surgical treatment of primary medisatinal tumors. Methods Clinical data were collected from a prospective database between January 2000 and January 2014. The analyses were mainly focused on the long-term survival of 190 cases that underwent radical resectioning surgeries. Results The three most common mediastinal tumors are thymic epithelial tumors in 95 cases (50%), neurogenic tumors in 26 cases (13.7%), and mediastinal germ cell tumors in 26 cases (13.7%). Of the 190 patients, 179 patients achieved the R0 resection criterion (94.2%), 8 underwent R2 resectioning (4.2%) and 3 underwent only exploration (1.6%), with 2 cases of death in the 30 days after the surgery. The 1-, 3-, and 5-year survival rates of the thymic epithelial tumor patients were 95%, 92.7%, and 85.7%, respectively. According to the Masaoka-Koga staging, the 5-year survival rates of stage Ⅰ, Ⅱ, Ⅲ, and Ⅳ thymic epithelial tumors are 100%, 82.1%, 90%, and 37.5%, respectively. A multivariate analysis reveals that the Masaoka-Koga staging of thymic epithelial tumors is an independent prognostic factor (P < 0.05). According to pathological classification, the 5-year survival rates for A+AB+B1 versus B2+B3 type thymoma were 88.6% versus 76.9%, which is statistically significant (P < 0.05). Most of the neurogenic tumors are benign, all suffer R0 resectioning, and have long term survival. Conclusion Due to the complexity caused by its histology, the treatment of mediastinal tumors should be based on the origin, nature, location, and size of the tumors. Although the patients of the group have a favorable prognosis, it is difficult to draw conclusions from the studies because of its retrospective characteristics and small sample size. Therefore, to get better clinical evidence, a multi-center, large sample, and prospective clinical study should be performed. -
Key words:
- Primary mediastinal tumor /
- thymic epithelial tumour /
- surgery /
- survival
-

图 1 Masaoka-Koga不同分期患者的生存率比较
Figure 1. Comparison of the overall survival curves of the thymic epithelial tumors according to the Masaoka-Koga staging

图 2 不同胸腺瘤WHO病理分类患者的生存率比较
Figure 2. Comparison of the overall survival curves for thymoma according to the WHO classification

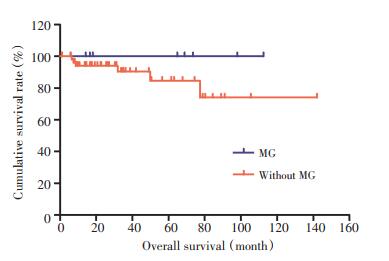
图 3 胸腺瘤是否合并重症肌无力患者生存比较
Figure 3. Comparison of the overall survival curves for thymoma with or without myasthenia gravis(MG)
表 1 190例原发纵隔肿瘤病理分类
Table 1. Pathological classification of 190 patients with primary mediasti nal tumors

表 2 190例原发性纵隔肿瘤治疗资料
Table 2. Treatment characteristics of 190 patients with primary mediastinal tumors

-
[1] Travis WD, Brambilla E, Muller-Hermelink H, et al. Pathology and genetics of tumors of the lung, pleura, thymus and heart[M]. In Kleihues P, Sobin Ls. WHO Classification of Tumors, 2nd Ed. Lyon, IARC Press, 2004: 145-197. [2] Koga K, Matsuno Y, Noguchi M, et al. A review of 79 thymomas: modification of staging system and reappraisal of conventional division into invasive and non-invasive thymoma[J]. Pathol Int, 1994, 44(5):359-367. http://cn.bing.com/academic/profile?id=1b7d452c07b5c0ce97e29f624af53c8b&encoded=0&v=paper_preview&mkt=zh-cn [3] Fang WT, Xu MY, Chen G, et al. Minimally invasive approaches for histological diagnosis of anterior mediastinal masses.[J]. Chin Med J (Engl), 2007, 120(8):675-679. doi: 10.1097/00029330-200704020-00012 [4] 张志庸, 主编.现代实用纵隔外科学[M].北京: 中国协和医科大学出版社, 2008: 301-302.Zhang ZY. Modern practical mediastinal surgery[M]. Peking Union Medical College Press, 2008: 301-302. [5] Sarkaria IS, Bains MS, Sood S, et al. Resection of primary mediastinal non-seminomatous germ cell tumors: a 28-year experience at memorial sloan-kettering cancer center[J]. J Thorac Oncol, 2011, 6 (7):1236-1241. doi: 10.1097/JTO.0b013e31821d513e [6] Pennathur A, Qureshi I, Schuchert MJ, et al. Comparison of surgical techniques for early-stage thymoma: feasibility of minimally invasive thymectomy and comparison with open resection[J]. J Thorac Cardiovasc Surg, 2011, 141(3):694-701. doi: 10.1016/j.jtcvs.2010.09.003 [7] Aydiner A, Toker A, Sen F, et al. Association of clinical and pathological variables with survival in thymoma[J]. Med Oncol (Northwood, London, England), 2012, 29(3):2221-2228. doi: 10.1007/s12032-011-0101-z [8] Detterbeck FC. Evaluation and treatment of stageⅠ and Ⅱ thymoma[J]. J Thorac Oncol, 2010, 5(10):S318-S322. doi: 10.1097/JTO.0b013e3181f20dab [9] Anile M, Patella M, Venuta F. The role of postoperative radiotherapy after resection of stage Ⅲ thymoma[J]. J Thorac Oncol, 2011, 6 (12):2142-2143. doi: 10.1097/JTO.0b013e318236e3af [10] Ried M, Potzger T, Sziklavari Z, et al. Extended surgical resections of advanced thymoma Masaoka-Stages Ⅲ and IVa facilitate outcome[J]. Thorac Cardiovasc Surg, 2013, 17:[Epub ahead of print]. https://pubmed.ncbi.nlm.nih.gov/23775415/ [11] Venuta F, Rendina EA, Anile M, et al. Thymoma and thymic carcinoma[J]. Gen Thorac Cardiovasc Surg, 2012, 60(1):1-12. http://cn.bing.com/academic/profile?id=12237d8353d9a97de7ac3816e0e31fb7&encoded=0&v=paper_preview&mkt=zh-cn [12] Girard N, Lal R, Wakelee H, et al. Chemotherapy definitions and policies for thymic malignancies[J]. J Torac Oncol, 2011, 6(7suppl 3):S1739-S1755. http://cn.bing.com/academic/profile?id=ca05c9fe9ae37f390bcff92c41e7de57&encoded=0&v=paper_preview&mkt=zh-cn [13] Patel S, Macdonald OK, Nagda S, et al. Evaluation of the role of radiation therapy in the management of malignant thymoma[J]. Int J Radiat Oncol Biol Phys, 2012, 82(5):1797-1801. doi: 10.1016/j.ijrobp.2011.03.010 [14] 杨异, 陈文虎, 吉春宇, 等.原发于纵隔的淋巴瘤外科治疗分析[J].中华胸心血管外科杂志, 2002, 18(5):315. doi: 10.3760/cma.j.issn.1001-4497.2002.05.028Yang Y, Chen WH, Ji CY, et al. Analysis of surgical treatment of primary mediastinal lymphoma[J]. Chin J Thor Card Surg, 2002, 18 (5):315. doi: 10.3760/cma.j.issn.1001-4497.2002.05.028 [15] Ricci C, Rendina EA, Venuta F, et al. Surgical approach to isolated mediastinal lymphoma[J]. J Thorac Cardiovasc Surg, 1990, 99(4): 691-695. doi: 10.1016/S0022-5223(19)36945-4 -

 下载:
下载:
 点击查看大图
点击查看大图

计量
- 文章访问数: 33
- HTML全文浏览量: 22
- PDF下载量: 0
- 被引次数: 0
