
Chemotherapy for metastatic colorectal cancer after failure of treatment with irinotecan and oxaliplatin
-
摘要:
目的 通过回顾性分析奥沙利铂及伊立替康化疗失败的转移性结直肠癌化疗疗效,探索结直肠癌的解救化疗方案。 方法 回顾2005年1月~2013年3月本院经奥沙利铂及伊立替康化疗失败的转移性结直肠癌患者37例,分析化疗的有效率(RR)及无进展生存(PFS)。 结果 化疗总有效率13.51%(5/37),5例PR,12例SD,20例PD;以培美曲塞为基础化疗方案总有效率略高于其他方案(17.64% vs. 10.00%,P=0.64),未延长PFS(2.00个月vs. 1.63个月,HR=0.79,95%CI:0.35~1.78,P=0.58);以雷替曲塞为基础的化疗方案有效率略高于其他方案(16.67% vs. 12.00%,P=0.34),未延长PFS(1.58个月vs. 1.90个月,HR=2.24,95%CI:0.98~5.12,P=0.06)。 结论 以培美曲塞或雷替曲塞为基础的联合化疗方案对奥沙利铂及伊立替康化疗失败的转移性结直肠癌患者有一定疗效,值得进一步开展临床研究。 Abstract:Objective This retrospective study aims to determine the efficacy of chemotherapy and improve a salvage chemotherapy agent for metastatic colorectal cancer (MCRC) after failure of treatment with irinotecan and oxaliplatin. Methods Between January 2002 and March 2013, 37 patients with metastatic MCRC who had progressed after treatment with irinotecan and oxaliplatin were analyzed for their response rate (RR) and progression-free survival (PFS). Results The overall RR of the 37 patients was 13.51%, with 5 cases of partial response (PR), 12 cases of disease stabilization (SD), and 20 cases of progression (PD). Compared with other chemotherapy regimens, treatment with a pemetrexed-based chemotherapy agent had a higher RR (17.64% vs. 10.00%, P=0.64) without a longer PFS (2.00 months vs. 1.63 months, HR=0.79, 95%, CI: 0.35 to 1.78, P=0.58). Compared with other chemotherapy regimens, treatment with a raltirexed-based chemotherapy agent had a higher RR (16.67% vs. 12.00%, P=0.34) without a longer PFS (1.58 months vs. 1.90 months, HR=2.24, 95%, CI: 0.98 to 5.12, P=0.06). Conclusion In patients with MCRC after failure of treatment with irinotecan and oxaliplatin, a pemetrexed-based or raltirexed-based chemotherapy agent may beneficial during salvage treatment and is therefore worthy of further study. -
Key words:
-
/ - colorectal cancer /
- salvage chemotherapy agent /
- oxaliplatin pemetrexed
-
-

图 1 以培美曲塞为基础化疗方案的无进展生存曲线
Figure 1. PFS of patients treated with pemetrexed-based chemotherapy and other agent

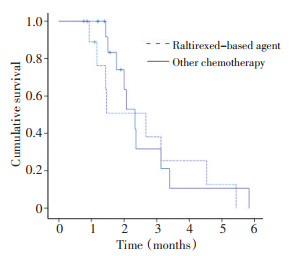
图 2 以雷替曲塞为基础化疗方案的无进展生存曲线
Figure 2. PFS of patients treated with raltirexed-based chemotherapy and other agent
表 1 临床及病理特征 例(%)
Table 1. Clinical and pathologic of characteristics (n%)

表 2 转移性结、直肠癌的治疗方案 例(%)
Table 2. Chemotherapy regimens for metastatic colorectal cancer (n%)

表 3 不良反应分级
Table 3. Toxicity profile by grade

-
[1] Gill S, Thomas RR, Goldbeg RM. Review article: colorectal cancer chemotherapy[J]. Aliment Pharmacil Ther, 2003, 18(7): 683-692. doi: 10.1046/j.1365-2036.2003.01735.x [2] Midigley R, Kerr D. colorectal cancer[J]. Lancet, 1999, 353(9150): 391-399. doi: 10.1016/S0140-6736(98)07127-X [3] 赵平, 陈万青, 雷正龙. 中国肿瘤登记年报(2009)[M]. 北京: 军事医学科学出版社, 2010: 26-30. [4] Venook A. Critical evaluation of current treatments in metastatic colorectal[J]. Oncologist, 2005, 10(4): 250-261. doi: 10.1634/theoncologist.10-4-250 [5] Bitossi R, Sculli CM, Tampellini M, et al. Gemcitabine and protracted 5-fluorouracil infusion as third-line chemotherapy in refractory colorectal cancer patients[J]. Anticancer Res, 2008, 28(5B): 3055-3060. [6] Bendell JC, Nemunaitis J, Vukelja SJ, et al. Randomized placebo-controlled phase Ⅱ trial of perifosine plus capecitabine as second- or third-line therapy in patients with metastatic colorectal cancer[J]. J Clin Oncol, 2011, 29(33): 4394-4400. doi: 10.1200/JCO.2011.36.1980 [7] Scartozzi M, Falcone A, Pucci F, et al. Capecitabine and mitomycin C may be an effective treatment option for third-line chemotherapy in advanced colorectal cancer[J]. Tumori, 2006, 92(5): 384-388. doi: 10.1177/030089160609200503 [8] Wu XY, Huang XE, You SX, et al. Phase Ⅱ Study of Pemetrexed as Second or Third Line Combined Chemotherapy in Patients with Colorectal Cancer[J]. Asian Pac J Cancer Prev, 2013, 14(3): 2019-2022. doi: 10.7314/APJCP.2013.14.3.2019 [9] Yasui H, Yoshino T, Boku N, et al. Retrospective analysis of S-1 monotherapy in patients with metastatic colorectal cancer after failure to fluoropyrimidine and irinotecan or to fluoropyrimidine, irinotecan and oxaliplatin[J]. Jpn J Clin Oncol, 2009, 39(5): 315-320. doi: 10.1093/jjco/hyp014 [10] Kim JH, Kim HS, Choi DR, et al. A phase Ⅱ study of mitomycin-C and S-1 as third-line chemotherapy in patients with advanced colorectal cancer[J]. Oncol Lett, 2011, 2(6): 1253-1256. doi: 10.3892/ol.2011.367 [11] Gravalos C, Salut A, García-Girón C, et al. A randomized phase Ⅱ study to compare oxaliplatin plus 5-fluorouracil and leucovorin (FOLFOX4) versus oxaliplatin plus raltitrexed (TOMOX) as first-line chemotherapy for advanced colorectal cancer[J]. Clin Transl Oncol, 2012, 14(8): 606-612. doi: 10.1007/s12094-012-0843-x [12] Rosati G, Rossi A, Germano D, et al. Raltitrexed and mitomycin-C as third-line chemotherapy for colorectal cancer after combination regimens including 5-fluorouracil, irinotecan and oxaliplatin: a phase Ⅱ study[J]. Anticancer Res, 2003, 23(3C): 2981-2985. [13] Pfeiffer P, Nielsen D, Bjerregaard J, et al. Biweekly cetuximab and irinotecan as third-line therapy in patients with advanced colorectal cancer after failure to irinotecan, oxaliplatin and 5-fluorouracil[J]. Ann Oncol, 2008, 19(6): 1141-1145. doi: 10.1093/annonc/mdn020 [14] Spindler KL, Pallisgaard N, Lindebjerg J, et al. EGFR related mutational status and association to clinical outcome of third-line cetuximab-irinotecan in metastatic colorectal cancer[J]. BMC Cancer, 2011, 11: 107. doi: 10.1186/1471-2407-11-107 [15] Park LC, Lee HS, Shin SH, et al. Bevacizumab as a second-or lat er-line of treatment for metastatic colorectal cancer[J]. World J Gastroenterol, 2012, 18(10): 1104-1109. doi: 10.3748/wjg.v18.i10.1104 [16] Kaneko J, Isogai J, Aoyagi H, et al. A case of unresectable multiple hepatic metastases from colorectal cancer successfully treated with panitumumab therapy on third-line[J]. Gan To Kagaku Ryoho, 2011, 38(12): 2247-2249. -

 下载:
下载:
 点击查看大图
点击查看大图

计量
- 文章访问数: 178
- HTML全文浏览量: 95
- PDF下载量: 2
- 被引次数: 0
