
Effects of arsenic trioxide combined with first-line chemotherapy on osteosarcoma of patients with pulmonary extremity metastasis
-
摘要:
目的 通过回顾北京大学人民医院骨与软组织肿瘤中心十年以上的肢体骨肉瘤肺转移的病例,对其预后、治疗过程进行总结,以期发现三氧化二砷(arsenic trioxide,ATO)联合一线化疗药物对早期肺转移病例的疗效。 方法 回顾性分析北京大学人民医院骨肿瘤科自1998年3月至2014年12月收治的肢体骨肉瘤肺转移的连续病例,挑选出治疗过程中出现早期肺转移及初治肺转移曾经使用过ATO长期输液联合一线化疗药物(阿霉素、顺铂、大剂量氨甲喋呤和异环磷酰胺)进行治疗的病例。共计119例符合本研究条件,65例为初治肺转移,54例为治疗过程中发现肺转移。 结果 该组的病例经治疗,2年及5年总生存率分别为52.6%和30.9%。虽然仅20例接受了肺部切除手术(16.8%),但本中心选择治疗后的病例5年总生存情况和国际上其他区域的的生存情况类似(意大利Rizzoli的5年生存率为37%)。通过比较各项临床病理学因素,发现骨转移、双侧肺转移、出现≥3个肺转移结节以及不完全切除肺内病灶,提示患者预后不佳。 结论 ATO合并一线化疗可能是一种有效且患者可耐受的新的治疗选择。肺切除手术应该严格挑选合适的病例,以获得最大的临床受益。 Abstract:Objective After establishing standard multi-modal therapy, prognosis of refractory and metastatic high-grade osteosarcoma remains dismal and unchanged over the last decades. Early clinical intervention to newly detected metastatic lesions is crucial and effective for better prognosis. Arsenic trioxide (ATO) is one of the oldest remedies used in traditional oriental medicine and is recently rediscovered as an immunomodulator due to its activity against other solid tumors. This study aims to evaluate the efficiency of ATO combined with first-line chemotherapy in treating pulmonary metastatic osteosarcoma patients with long-term follow-up in our institution. Methods Osteosarcoma patients with pulmonary metastasis were intravenously administered with ATO (5-10 mg) daily combined with first-line chemotherapy for their treatment. A total of 119 patients were finally enrolled; 65 presented metastasis, and 54 relapsed with lung metastasis. Results Two-year and five-year overall survival (OS) rates for these patients reached 52.6% and 30.9%, respectively. Only 20 cases underwent thoracotomies (16.8%). Our five-year OS was nearly similar to that of other institutions (37% in Rizzoli, Italy). We observed that combined with bone metastasis, bilateral metastasis, and > 3 pulmonary nodules, incomplete resection of pulmonary lesions deteriorated the disease and significantly influenced survival as compared with all other parameters. Conclusion Combined with conventional chemotherapy, ATO may be effective and well-tolerated as new therapeutic option for patients with nonresectable pulmonary metastatic osteosarcoma. Lung metastasectomy should be strictly selected only for populations who benefit from this treatment. -
Key words:
- osteosarcoma /
- pulmonary metastasis /
- arsenic trioxide /
- first-line chemotherapy
-

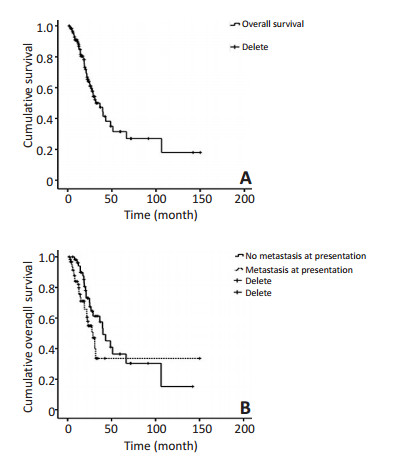
图 1 患者的Kaplan-Meier生存曲线
Figure 1. Patients' Kaplan-Meier survival curves
A. Overall survival of all patients; B. Overall survival of patients who had metastasis at presentation and who relapsed with pulmonary metastasis

图 2 生存时间 > 10年的24岁骨肉瘤患者的肺部CT表现
Figure 2. The chest CT of a 24-year old patient who survived longer than ten years following this chemo-protocol (multiple calcifications in relation to metastatic lesions)
A. The chest CT taken in 2003; B. The chest CT taken in 2013
表 1 本研究中患者的临床病理学参数
Table 1. Characteristics of the patients reviewed in this study

-
[1] Luetke A, Meyers PA, Lewis I, et al. Osteosarcoma treatmentwhere do we stand? A state of the art review[J]. Cancer Treat Rev, 2014, 40(4):523-532. doi: 10.1016/j.ctrv.2013.11.006 [2] Jaffe N, Puri A, Gelderblom H, et al. Osteosarcoma: evolution of treatment paradigms[J]. Sarcoma, 2013, 2013:203531. https://www.hindawi.com/journals/sarcoma/2013/203531/ [3] Meyers PA, Chou AJ. Muramyl tripeptide-phosphatidyl ethanolamine encapsulated in liposomes (L-MTP-PE) in the treatment of osteosarcoma[J]. Adv Exp Med Biol, 2014, 804:307-321. doi: 10.1007/978-3-319-04843-7 [4] Whelan JS, Bielack SS, Marina N, et al. EURAMOS-1, an international randomised study for osteosarcoma: results from pre-randomisation treatment[J]. Ann Oncol, 2015, 26(2):407-414. doi: 10.1093/annonc/mdu526 [5] Sui M, Zhang Z, Zhou J, et al. Inhibition factors of arsenic trioxide therapeutic effects in patients with acute promyelocytic leukemia [J]. Chin Med J (Engl), 2014, 127(19):3503-3506. https://www.researchgate.net/publication/266379747_Inhibition_factors_of_arsenic_trioxide_therapeutic_effects_in_patients_with_acute_promyelocytic_leukemia [6] Efficace F, Mandelli F, Avvisati G, et al. Randomized phase Ⅲ trial of retinoic acid and arsenic trioxide versus retinoic acid and chemotherapy in patients with acute promyelocytic leukemia: health-related quality-of-life outcomes[J]. J Clin Oncol, 2014, 32(30):3406-3412. doi: 10.1200/JCO.2014.55.3453 [7] Wang H, Cao F, Li J, et al. Arsenic trioxide and mannitol for the treatment of acute promyelocytic leukemia relapse in the central nervous system[J]. Blood, 2014, 124(12):1998-2000. doi: 10.1182/blood-2014-04-568121 [8] Thomas-Schoemann A, Batteux F, Mongaret C, et al. Arsenic trioxide exerts antitumor activity through regulatory T cell depletion mediated by oxidative stress in a murine model of colon cancer[J]. J Immunol, 2012, 189(11):5171-5177. doi: 10.4049/jimmunol.1103094 [9] Griffin RJ, Williams BW, Park HJ, et al. Preferential action of arsenic trioxide in solid-tumor microenvironment enhances radiation therapy[J]. Int J Radiat Oncol Biol Phys, 2005, 61(5):1516-1522. doi: 10.1016/j.ijrobp.2004.12.058 [10] Tingting R, Wei G, Changliang P, et al. Arsenic trioxide inhibits osteosarcoma cell invasiveness via MAPK signaling pathway[J]. Cancer Biol Ther, 2010, 10(3):251-257. doi: 10.4161/cbt.10.3.12349 [11] Yang GF, Li XH, Zhao Z, et al. Arsenic trioxide up-regulates Fas expression in human osteosarcoma cells[J]. Chin Med J (Engl), 2010, 123(13):1768-1773. https://www.ncbi.nlm.nih.gov/pubmed/20819644 [12] Duffaud F, Therasse P. New guidelines to evaluate the response to treatment in solid tumors[J]. Bull Cancer, 2000, 87(12):881-886. https://www.ncbi.nlm.nih.gov/pubmed?term=%22Journal+of+the+National+Cancer+Institute%22%5BJour%5D+AND+92%5Bvolume%5D+AND+205%5Bpage%5D+AND+2000%5Bpdat%5D&cmd=detailssearch [13] Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada[J]. J Natl Cancer Inst, 2000, 92(3):205-216. doi: 10.1093/jnci/92.3.205 [14] Schindler B, Briel M, Gunther J, et al. Painting by number--Survival curves and Kaplan-Meier method[J]. Med Monatsschr Pharm, 2015, 38(5):186-191. https://www.ncbi.nlm.nih.gov/pubmed/26364408 [15] Alberti C, Timsit JF, Chevret S. Survival analysis-the log rank test[J]. Rev Mal Respir, 2005, 22(5 Pt 1):829-832. https://www.slideshare.net/zhe1/kaplan-meier-survival-curves-and-the-logrank-test [16] Bielack S, Carrle D, Casali PG, et al. Osteosarcoma: ESMO clinical recommendations for diagnosis, treatment and follow-up[J]. Ann Oncol, 2009, 20 Suppl 4:137-139. https://www.ncbi.nlm.nih.gov/pubmed/17491058 [17] Kager L, Zoubek A, Potschger U, et al. Primary metastatic osteosarcoma: presentation and outcome of patients treated on neoadjuvant cooperative osteosarcoma study group protocols[J]. J Clin Oncol, 2003, 21(10):2011-2018. doi: 10.1200/JCO.2003.08.132 [18] Geller DS, Gorlick R. Osteosarcoma: a review of diagnosis, management, and treatment strategies[J]. Clin Adv Hematol Oncol, 2010, 8 (10):705-718. https://www.researchgate.net/publication/49832983_Osteosarcoma_A_review_of_diagnosis_management_and_treatment_strategies [19] Kempf-Bielack B, Bielack SS, Jurgens H, et al. Osteosarcoma relapse after combined modality therapy: an analysis of unselected patients in the Cooperative Osteosarcoma Study Group (COSS)[J]. J Clin Oncol, 2005, 23(3):559-568. doi: 10.1200/JCO.2005.04.063 [20] Bacci G, Rocca M, Salone M, et al. High grade osteosarcoma of the extremities with lung metastases at presentation: treatment with neoadjuvant chemotherapy and simultaneous resection of primary and metastatic lesions[J]. J Surg Oncol, 2008, 98(6):415-420. doi: 10.1002/jso.v98:6 [21] Carrle D, Bielack S. Osteosarcoma lung metastases detection and principles of multimodal therapy[J]. Cancer Treat Res, 2009, 152: 165-184. doi: 10.1007/978-1-4419-0284-9 [22] Hoefnagel CA, Bruning PF, Cohen P, et al. Detection of lung metastases from osteosarcoma by scintigraphy using 99mTc-methylene diphosphonate[J]. Diagn Imaging, 1981, 50(5):277-284. https://www.ncbi.nlm.nih.gov/pubmed/6457735 [23] Briccoli A, Rocca M, Salone M, et al. High grade osteosarcoma of the extremities metastatic to the lung: long-term results in 323 patients treated combining surgery and chemotherapy, 1985-2005[J]. Surg Oncol, 2010, 19(4):193-199. doi: 10.1016/j.suronc.2009.05.002 [24] Steliga M, Vaporciyan A. Surgical treatment of pulmonary metastases from osteosarcoma in pediatric and adolescent patients[J]. Cancer Treat Res, 2009, 152:185-201. doi: 10.1007/978-1-4419-0284-9 [25] Bacci G, Ferrari S, Longhi A, et al. Therapy and survival after recurrence of Ewing's tumors: the Rizzoli experience in 195 patients treated with adjuvant and neoadjuvant chemotherapy from 1979 to 1997[J]. Ann Oncol, 2003, 14(11):1654-1659. doi: 10.1093/annonc/mdg457 [26] Bacci G, Forni C, Ferrari S, et al. Neoadjuvant chemotherapy for osteosarcoma of the extremity: intensification of preoperative treatment does not increase the rate of good histologic response to the primary tumor or improve the final outcome[J]. J Pediatr Hematol Oncol, 2003, 25(11):845-853. doi: 10.1097/00043426-200311000-00006 [27] Anninga JK, Gelderblom H, Fiocco M, et al. Chemotherapeutic adjuvant treatment for osteosarcoma: where do we stand[J]? Eur J Cancer, 2011, 47(16):2431-2445. doi: 10.1016/j.ejca.2011.05.030 [28] Harting MT, Blakely ML, Jaffe N, et al.Long-term survival after aggressive resection of pulmonary metastases among children and adolescents with osteosarcoma[J]. J Pediatr Surg, 2006, 41(1):194-199. doi: 10.1016/j.jpedsurg.2005.10.089 [29] Chen YB, Hahn LJ, Yao YT.Long-term survival of mandibular osteosarcoma[J]. Br J Plast Surg, 1999, 52(3):243-244. https://www.ncbi.nlm.nih.gov/pubmed/10474489 [30] Shibamoto Y, Horii N, Takahashi M. Long-term control of multiple lung metastases from osteosarcoma obtained by conventional radiotherapy: a case report[J]. Oncol Rep, 1999, 6(5):1085-1087. https://www.spandidos-publications.com/or/6/5/1085/abstract -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 64
- HTML全文浏览量: 9
- PDF下载量: 1
- 被引次数: 0
