
Relationship between preoperative FIB-4 and hepatocellular carcinoma prognosis after curative resection
-
摘要:
目的 探讨FIB(Fibrosis)-4评分系统与肝细胞癌(HCC)患者临床病理特征及预后的关系。 方法 收集2009年1月至2012年12月间245例接受根治性肝切除手术的HCC患者的临床及随访资料进行分析,利用Kaplan-Meier进行单因素生存分析,Cox比例风险回归模型进行多因素生存分析。 结果 根据患者术前FIB-4评分,将患者分为FIB-4Ⅰ(≤3.25)和FIB-4Ⅱ( > 3.25)。FIB-4能够预测肝硬化程度(Ishak分级:1~5级 vs. 6级,r=0.681,P < 0.001),其主要与患者的肝功能指标如谷草转氨酶(P < 0.001)、胆红素(P=0.009)、白蛋白(P=0.001)及血小板计数(P < 0.001)相关,与其他病理特征无关。单因素及多因素分析均表明FIB-4能够预测HCC患者的预后(总生存时间:P=0.037,0.011;无瘤生存时间:P=0.027,0.043)。 结论 FIB-4有可能作为HCC根治性切除术后的预后参考指标之一。 Abstract:Objective To investigate the correlation between FIB-4 and the clinicopathological characteristics and prognosis of patients with hepatocellular carcinoma (HCC) after curative resection. Methods From January 2009 to December 2012, the clinicopathological and follow-up data of 245 patients with HCC after curative resection were retrospectively studied. Their survival was calculated using the Kaplan-Meier method. The Cox proportional hazard regression model was used for the multivariate analysis. Results According to FIB-4 index, patients were divided into two subgroups: FIB-4Ⅰ(≤3.25) and FIB-4Ⅱ( > 3.25). FIB-4 could predict liver cirrhosis severity (Ishak grade, Grade 1-5 vs. Grad 6, r=0.681, P < 0.001). It was associated with liver function such as:aspartate transaminase (P < 0.001)、total bilirubin (P=0.009)、albumin (P=0.001) and platelet count (P < 0.001) other than tumor clinicopathologic features. Both univariate and multivariate analysis showed FIB-4 could predict the prognosis of HCC patients (Overall survival: P=0.037 and 0.011; Recurrencefree survival: P=0.027 and P=0.043, respectively). Conclusion The preoperative FIB-4 index could be used as a prognostic marker for the prognosis of HCC after curative hepatectomy. -
Key words:
- hepatocellular carcinoma /
- liver cirrhosis /
- FIB-4 /
- hepatitis B virus /
- prognosis
-

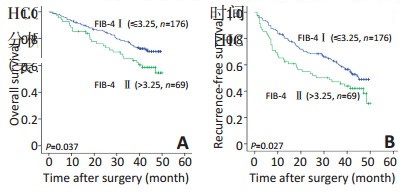
图 1 肝细胞癌患者的生存曲线
Figure 1. Overall survival (A) and recurrence-free survival (B) curves of patients with hepatocellular carcinoma
A. OS; B. RFS
表 1 肝细胞癌患者的临床病理特征
Table 1. Clinical characteristics of patients with hepatocellular carcinoma

表 2 患者总生存时间和无瘤生存时间的单因素和多因素分析
Table 2. Univariate and multivariate analyses for the overall and recurrence free survival of patients

表 3 高FIB-4评分组( > 3.25,n=69)的预后分析
Table 3. Prognostic analyses of high FIB-4 scoring subgroup ( > 3.25, n=69)

-
[1] Wei KR, Yu X, Zheng RS, et al.Incidence and mortality of liver cancer in China, 2010[J]. Chin J Cancer, 2014, 33(8):388-394. doi: 10.1186/s40880-015-0056-0 [2] Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017[J]. CA Cancer J Clin, 2017, 67(1):7-30. doi: 10.3322/caac.21387 [3] Sia D, Villanueva A, Friedman SL, et al.Liver Cancer cell of origin, molecular class, and effects on patient prognosis[J]. Gastroenterology, 2017, 152(4):745-761. doi: 10.1053/j.gastro.2016.11.048 [4] Chen MM, Xiao X, Lao XM, et al. Polarization of tissue-resident TFHlike cells in human hepatoma bridges innate monocyte inflammation and M2b macrophage polarization[J]. Cancer Discov, 2016, 6 (10):1182-1195. doi: 10.1158/2159-8290.CD-16-0329 [5] 唐涛, 廖锐, 李静, 等.肝细胞癌患者根治性切除术后的预后因素分析[J].中华外科杂志, 2016, 54(6):439-443. http://cdmd.cnki.com.cn/Article/CDMD-12121-1016267844.htmTang T, Liao R, Li J, et al. Analysis of prognostic factors of patients with hepatocellular carcinoma after radical resection[J]. Chin J Surg, 2016, 54(6):439-443. http://cdmd.cnki.com.cn/Article/CDMD-12121-1016267844.htm [6] Wang Q, Fiel MI, Blank S, et al. Impact of liver fibrosis on prognosis following liver resection for hepatitis B-associated hepatocellular carcinoma[J]. Br J Cancer, 2013, 109(3):573-581. doi: 10.1038/bjc.2013.352 [7] Jung KS, Kim SU, Choi GH, et al. Prediction of recurrence after curative resection of hepatocellular carcinoma using liver stiffness measurement (FibroScan®)[J]. Ann Surg Oncol, 2012, 19(13):4278-4286. doi: 10.1245/s10434-012-2422-3 [8] Yin Z, Zou J, Li Q, et al. Diagnostic value of FIB-4 for liver fibrosis in patients with hepatitis B: a meta-analysis of diagnostic test[J]. Oncotarget, 2017. doi: 10.18632/oncotarget.14430. [9] Vallet-Pichard A, Mallet V, Nalpas B, et al. FIB-4: an inexpensive and accurate marker of fibrosis in HCV infection. comparison with liverbiopsy and fibrotest[J]. Hepatology, 2007, 46(1):32-36. doi: 10.1002/(ISSN)1527-3350 [10] 郭剑洋, 杜成友, 李德卫, 等.肝切除术中单用双极电凝断肝的临床研究[J].中华外科杂志, 2014, 52(7):547-550. http://cdmd.cnki.com.cn/Article/CDMD-10631-1014409093.htmGuo JY, Du CY, Li DW, et al. Clinical research of saline-coupled bipolar electrocautery for hepatic transection[J]. Chin J Surg, 2014, 52 (7):547-550. http://cdmd.cnki.com.cn/Article/CDMD-10631-1014409093.htm [11] Toyoda H, Kumada T, Tada T, et al. A laboratory marker, FIB-4 index, as a predictor for long-term outcomes of hepatocellular carcinoma patients after curative hepatic resection[J]. Surgery, 2015, 157(4): 699-707. doi: 10.1016/j.surg.2014.10.022 [12] Bruix J, Gores GJ, Mazzaferro V.Hepatocellular carcinoma: clinical frontiers and perspectives[J]. Gut, 2014, 63(5):844-855. doi: 10.1136/gutjnl-2013-306627 [13] 罗斌, 阙祖俊, 田建辉.髓源性抑制细胞促进循环肿瘤细胞形成转移的研究进展[J].中国肿瘤临床, 2016, 43(11):493-497. doi: 10.3969/j.issn.1000-8179.2016.11.203Luo B, Que ZJ, Tian JH. Progress on metastasis induced by myeloidderived suppressor cells to promote circulating tumor cell[J]. Chin J Clin Oncol, 2016, 43(11):493-497. doi: 10.3969/j.issn.1000-8179.2016.11.203 [14] Arzumanyan A, Reis HM, Feitelson MA. Pathogenic mechanisms in HBV-and HCV-associated hepatocellular carcinoma[J]. Nat Rev Cancer, 2013, 13(2):123-135. doi: 10.1038/nrc3449 [15] Hanahan D, Robert A. Weinberg. Hallmarks of Cancer: The Next Generation[J]. Cell, 2011, 144(5):646-674. doi: 10.1016/j.cell.2011.02.013 [16] Kim WR, Berg T, Asselah T, et al.Evaluation of APRI and FIB-4 scoring systems for non-invasive assessment of hepatic fibrosis in chronic hepatitis B patients[J]. J Hepatol, 2016, 64(4):773-780. doi: 10.1016/j.jhep.2015.11.012 -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 74
- HTML全文浏览量: 3
- PDF下载量: 1
- 被引次数: 0
