
Clinicopathological characteristic analysis of tubular carcinoma of the breast: 94 cases
-
摘要:
目的 探讨乳腺小管癌的临床病理特征、影像学诊断、治疗和预后。 方法 收集2006年4月至2012年9月天津医科大学肿瘤医院经病理确诊的94例乳腺小管癌患者的临床资料,回顾性分析其临床病理、影像学特征及治疗与预后。 结果 94例乳腺小管癌患者中超声检查阳性率为74.5%(70/94),显著高于乳腺X线检查阳性率60.6%(57/94),二者比较差异具有统计学意义(P=0.043)。乳腺小管癌患者ER、PR阳性率较高,HER-2阳性率较低。乳腺小管癌单纯型PR阳性率95.2%(60/63)显著高于混合型的80.6%(25/31),混合型的HER-2阳性率37.9%(11/29)显著高于单纯型的17.7%(11/62),二者比较差异均具有统计学意义(均P < 0.05)。 结论 乳腺小管癌是一种恶性度较低的肿瘤,推荐以保乳治疗为主。因其淋巴结转移率较低,建议肿物较小、复发风险较低的患者可免除保乳术后放疗,但因存在一定的复发风险,术后影像学随访仍非常重要。 Abstract:Objective To explore clinicopathological features, imaging diagnosis, treatment, and prognosis of tubular carcinoma of the breast. Methods This retrospective study included 94 patients in Tianjin Medical University Cancer Institute and Hospital from 2006 to 2012 aged 27 years or older who were histologically diagnosed with tubular carcinoma of the breast. Collected data comprised clinical characteristics, histopathological features, and breast sonographic and mammographic features of patients. Results Positive rate of breast sonography reached 74.5% (70/94), which is significantly higher than that of breast mammography examination (60.6%, 57/94)(P=0.043). Patients in our study showed high estrogen-receptor (ER) and progesterone-receptor (PR) positive rate but low human epidermal growth factor receptor 2 (HER-2)-positive rate. PR-positive rate of pure tubular carcinoma totaled 95.2% (60/63), which is significantly higher than that of mixed tubular carcinoma (80.6%, 25/31). In mixed tubular carcinoma, positive rate of HER-2 expression reached 37.9% (11/29), which is significantly higher than that of pure tubular carcinoma (17.7%, 11/62). Differences between groups were statistically significant (P < 0.05). Conclusion Tubular carcinoma of the breast features potential malignancy and favorable prognosis. Therefore, breast conservation treatment is recommended. In view of low incidence of axillary node metastases, post-operative radiation therapy is considered unnecessary. However, tubular carcinoma yields a certain recurrence rate. Thus, follow-up imaging of contralateral breast remains significant. -
Key words:
- breast /
- tubular carcinoma /
- mammography /
- ultrasonography /
- prognosis
-

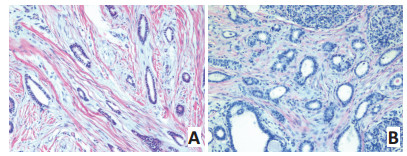
图 1 乳腺小管癌的病理组织学(H&E×200)
Figure 1. Histopathological features of tubular carcinoma of the breast (H&E×200)
A: Pure tubular carcinoma; B: Mixed tubular carcinoma
表 1 乳腺小管癌的影像学诊断
Table 1. Imaging diagnosis of tubular carcinoma of the breast

表 2 94例乳腺小管癌患者的单纯型及混合型临床病理特征
Table 2. Clinical and pathological features of 94 pure and mixed tubular carcinomas of the breast

-
[1] 李明, 王修珍.乳腺小管癌6例及文献复习[J].中国实用医药, 2011, 6 (9):182-183. http://www.cnki.com.cn/Article/CJFDTOTAL-ZSSA201109153.htmLi M, Wang XZ. Tubular carcinoma of the breast: a report of 6 cases and review of literature[J]. China Prac Med, 2011, 6(9):182-183. http://www.cnki.com.cn/Article/CJFDTOTAL-ZSSA201109153.htm [2] 曹薇, 徐灿, 高霭峰, 等.乳腺小管癌12例临床病理及免疫组织化学分析[J].中国组织化学与细胞化学杂志, 2010, 19(4):368-371. http://www.cnki.com.cn/Article/CJFDTOTAL-GGZZ201004011.htmCao W, Xu C, Gao AF. Clinicopathological and immunohistochemical analysis of 12 cases of tubular carcinoma of breast[J]. Chin J Histochemistry Cytochemistry, 2010, 19(4):368-371. http://www.cnki.com.cn/Article/CJFDTOTAL-GGZZ201004011.htm [3] Rakha EA, Lee AH, Evans AJ, et al. Tubular carcinoma of the breast: further evidence to support its excellent prognosis[J]. J Clin Oncol, 2010, 28(1): 99-104. doi: 10.1200/JCO.2009.23.5051 [4] Harvey JA. Unusual breast cancers: useful clues to expanding the differential diagnosis[J]. Radiology, 2007, 242(3):683-694. doi: 10.1148/radiol.2423051631 [5] Sheppard DG, Whitman GJ, Huynh PT, et al. Tubular carcinoma of the breast: mammographic and sonographic features[J]. AJR Am J Roentgenol, 2000, 174(1):253-257. doi: 10.2214/ajr.174.1.1740253 [6] Vilaverde F, Rocha A, Reis A. Tubular carcinoma of the breast: advantages and limitations of breast tomosynthesis[J]. Case Rep in Radiol, 2016, 2016: 3906195. [7] Oeffinger KC, Fontham ET, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American cancer society[J]. JAMA, 2015, 314(15):1599-1614. doi: 10.1001/jama.2015.12783 [8] Oakley GJ 3rd, Tubbs RR, Crowe J, et al. HER-2 amplification in tubular carcinoma of the breast[J]. Am J Clin Pathol, 2006, 126(1):55-58. doi: 10.1309/E0YEKHBP3YYQYUBD [9] Leonard CE, Howell K, Shapiro H, et al. Excision only for tubular carcinoma of the breast[J]. Breast J, 2005, 11(2):129-133. doi: 10.1111/tbj.2005.11.issue-2 [10] Boyan W, Shea B, Farr M, et al. Tubular carcinoma of the breast: a single institution's experience of a favorable prognosis[J]. Am Surg, 2016, 82(6):505-509. http://meetinglibrary.asco.org/content/154858-163 [11] Lea V, Gluch L, Kennedy CW, et al. Tubular carcinoma of the breast: axillary involvement and prognostic factors[J]. ANZ J Surg, 2015, 85 (6):448-451. doi: 10.1111/ans.2015.85.issue-6 [12] Kader HA, Jackson J, Mates D, et al. Tubular carcinoma of the breast: a population-based study of nodal metastases at presentation and of patterns of relapse[J]. Breast J, 2001, 7(1):8-13. doi: 10.1046/j.1524-4741.2001.007001008.x [13] Romano AM, Wages NA, Smolkin M. Tubular carcinoma of the breast: institutional and SEER database analysis supporting a unique classification[J]. Breast Dis, 2015, 35(2):103-111. doi: 10.3233/BD-140396 [14] Zandrino F, Calabrese M, Faedda C, et al. Tubular carcinoma of the breast: pathological, clinical, and ultrasonographic findings. A review of the literature[J]. Radiol Med, 2006, 111(6):773-782. doi: 10.1007/s11547-006-0071-y [15] Günhan-Bilgen I, Oktay A. Tubular carcinoma of the breast: mammographic, sonographic, clinical and pathologic findings[J]. Eur J of Radiol, 2007, 61(1):158-162. doi: 10.1016/j.ejrad.2006.08.021 -

 下载:
下载:
 点击查看大图
点击查看大图
图(1) / 表(2)
计量
- 文章访问数: 81
- HTML全文浏览量: 32
- PDF下载量: 1
- 被引次数: 0
