
-
摘要:
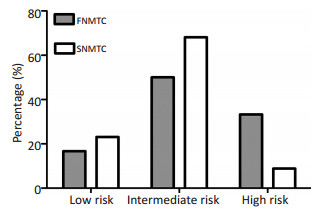
目的 探讨家族性非髓样甲状腺癌(familial non-medullary thyroid carcinoma,FNMTC)的临床特点。 方法 回顾性分析天津医科大学肿瘤医院2011年12月至2015年1月收治的10个不同家系24例FNMTC患者,对照组随机选择此期间182例散发性非髓样甲状腺癌(sporadic non-medullary thyroid carcinoma,SNMTC),对比家族性和散发性之间,家族性第一代与第二代之间临床病理学特征。包括年龄、性别、双侧、多灶性、腺外侵犯、淋巴结转移、是否伴发良性结节及桥本甲状腺炎、预后。 结果 FNMTC比SNMTC更易发生双侧病变(66.7% vs. 17.0%,P < 0.001),呈多灶性(45.8% vs. 25.8%,P < 0.050),伴发良性结节(70.8% vs. 40.7%,P < 0.010)和中央淋巴结转移(75.0% vs. 35.2%,P < 0.001)。家族性高危患者的比例高于散发组(33.3% vs. 8.8%,P < 0.05)。FNMTC中第二代患者疾病诊断年龄早于第一代[平均(45.6±10.3)vs.(35.3±5.4),P < 0.05]。 结论 双侧病变,多灶性,伴发良性结节和高中央淋巴结转移率是FNMTC的临床特征,其第二代患者疾病诊断年龄早于第一代。 -
关键词:
- 家族性非髓样甲状腺癌 /
- 多灶性 /
- 遗传早现
Abstract:Objective To analyze the clinicopathological features of familial non-medullary thyroid carcinoma (FNMTC). Methods A retrospective investigation was performed in 24 FNMTC patients from 10 families and 182 sporadic cases who were diagnosed and treated in Tianjin Medical University Cancer Institute and Hospital. Clinicopathological features were analyzed between familial group and sporadic group as well as between the first generation and the later generations of FNMTC patients. Results Compared with the patients with sporadic cancer, FNMTC patients were more likely to exhibit bilaterality (66.7% vs. 17.0%, P < 0.001), multifocality (45.8%vs. 25.8%, P=0.041), benign nodules (70.8% vs. 40.7%, P=0.005), and central lymph node metastasis (75.0% vs. 35.2%, P < 0.001). The proportion of American Thyroid Association (ATA) high-risk patients with FNMTC was higher than the sporadic group (33.3% vs. 8.8%, P=0.019). Comparison of the disease variants between the first generation and the later generations in FNMTC group showed that the latter were presented with disease at an earlier age at the time of diagnosis (mean 45.6±10.3 vs. 35.3±5.4, P=0.031). Conclusion Bilaterality, multifocality, presence of benign nodules, and central lymph node metastasis are special features of FNMTC. Moreover, the second generation has a younger age at the time of diagnosis compared with the first generation of FNMTC patients. -
Key words:
- familial non-medullary thyroid cancer /
- multifocality /
- anticipation
-

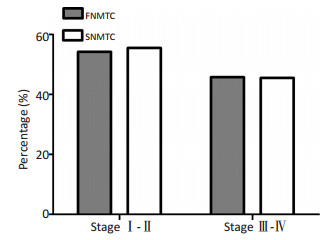
图 1 TNM分期
Figure 1. TNM staging
Stages Ⅰ-Ⅱ refers to TNMⅠ and Ⅱ, and stages Ⅲ-Ⅳ refers to TNM Ⅲ and Ⅳ. The percentage of TNM staging Ⅰ-Ⅱ in the familial group was 54.2% and 55.5% in the sporadic group
表 1 FNMTC与SNMTC临床病理特征
Table 1. Clinicopathological characteristics of the FNMTC group and SNMTC

表 2 FNMTC患者第一代和第二代临床病理学特点
Table 2. Clinicopathological characteristics of the first and second generations in FNMTC patients

-
[1] Charkes ND. On the prevalence of familial nonmedullary thyroid cancer in multiply affected kindreds[J]. Thyroid, 2006, 16(5):181-186. https://www.researchgate.net/publication/7165781_On_the_Prevalence_of_Familial_Nonmedullary_Thyroid_Cancer_in_Multiply_Affected_Kindreds [2] Musholt TJ, Musholt PB, Petrich T, et al. Familial papillary thyroid carcinoma: genetics, criteria for diagnosis, clinical features, and surgical treatment[J]. World J Surg, 2000, 24(11):1409-1417. doi: 10.1007/s002680010233 [3] Charkes ND. On the prevalence of familial nonmedullary thyroid cancer[J]. Thyroid, 1998, 8(9):857-858. doi: 10.1089/thy.1998.8.857 [4] Burgess JR, Duffield A, Wilkinson SJ, et al. Two families with an autosomal dominant inheritance pattern for papillary carcinoma of the thyroid[J]. J Clin Endocrinol Metab, 1997, 82(2):345-348. doi: 10.1210/jcem.82.2.3789 [5] Malchoff CD, Malchoff DM. Familial nonmedullary thyroid carcinoma[J]. Cancer Control, 2006, 13(2):106-110. http://www.medscape.com/viewarticle/536310_1 [6] Ito Y, Kakudo K, Hirokawa M, et al. Biological behavior and prognosis of familial papillary thyroid carcinoma[J]. Surgery, 2009, 145(1): 100-105. doi: 10.1016/j.surg.2008.08.004 [7] Loh KC. Familial nonmedullary thyroid carcinoma: a meta-review of case series[J]. Thyroid, 1997, 7(1):107-113. doi: 10.1089/thy.1997.7.107 [8] Kraimps JL, Bouin-Pineau MH, Amati P, et al. Familial papillary carcinoma of the thyroid[J]. Surgery, 1997, (121):715-718. https://www.ncbi.nlm.nih.gov/pubmed/3789026 [9] Grossman RF, Tu SH, Duh QY, et al. Familial nonmedullary thyroid cancer: an emerging entity that warrants aggressive treatment[J]. Arch Surg, 1995, 131(131):892-897. https://www.ncbi.nlm.nih.gov/pubmed/8645080 [10] Houlston RS, Stratton MR. Genetics of non-medullary thyroid cancer [J]. QJM, 1995, 88(10):685-693. https://www.cancer.gov/types/thyroid/hp/medullary-thyroid-genetics-pdq [11] Malchoff CD, Malchoff DM. Familial nonmedullary thyroid carcinoma[J]. Semin Surg Oncol, 1999, 16(1):6-8. http://www.medscape.com/viewarticle/536310_1 [12] Lesueur F, Stark M, Tocco T, et al. Genetic heterogeneity in familial nonmedullary thyroid carcinoma: exclusion of linkage to RET, MNG1, and TCO in 56 families. NMTC Consortium[J]. J Clin Endocrinol Metab, 1999, 84(6):2157-2162. https://utah.pure.elsevier.com/en/publications/genetic-heterogeneity-in-familial-nonmedullary-thyroid-carcinoma- [13] Triponez F, Wong M, Sturgeon C, et al. Does familial non-medullary thyroid cancer adversely affect survival[J]? World J Surg, 2006, 30 (5):787-793. doi: 10.1007/s00268-005-0398-x [14] Kandil E, Noureldine SI, Abbas A, et al. The impact of surgical volume on patient outcomes following thyroid surgery[J]. Surgery, 2013, 154(6):1346-1352. doi: 10.1016/j.surg.2013.04.068 [15] Pal T, Vogl FD, Chappuis PO, et al. Increased risk for nonmedullary thyroid cancer in the first degree relatives of prevalent cases of nonmedullary thyroid cancer: a hospital-based study[J]. J Clin Endocrinol Metab, 2001, 86(11):5307-5312. doi: 10.1210/jcem.86.11.8010 [16] Landgren O, Linet MS, McMaster ML, et al. Familial characteristics of autoimmune and hematologic disorders in 8 406 multiple myeloma patients: a population-based case-control study[J]. Int J Cancer, 2006, 118(118):3095-3098. doi: 10.1002/ijc.21745/full [17] Uchino S, Noguchi S, Yamashita H, et al. Detection of asymptomatic differentiated thyroid carcinoma by neck ultrasonographic screening for familial nonmedullary thyroid carcinoma[J]. World J Surg, 2004, 28(11):1099-1102. doi: 10.1007/s00268-004-7676-x [18] Popadich A, Levin O, Lee JC, et al. A multicenter cohort study of total thyroidectomy and routine central lymph node dissection for cN0 papillary thyroid cancer[J]. Surgery, 2011, 150(6): 1048-1057. doi: 10.1016/j.surg.2011.09.003 [19] Mulla M, Schulte KM. Central cervical lymph node metastases in papillary thyroid cancer: a systematic review of imaging-guided and prophylactic removal of the central compartment[J]. Clin Endocrinol (Oxf), 2012, 76(1):131-136. doi: 10.1111/cen.2011.76.issue-1 [20] Randolph GW, Duh QY, Heller KS, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension[J]. Thyroid, 2012, 22 (11):1144-1152. doi: 10.1089/thy.2012.0043 [21] Moo TA, McGill J, Allendorf J, et al. Impact of prophylactic central neck lymph node dissection on early recurrence in papillary thyroid carcinoma[J]. World J Surg, 2010, 34(6):1187-1191. doi: 10.1007/s00268-010-0418-3 [22] Takami H, Ito Y, Okamoto T, et al. Therapeutic strategy for differentiated thyroid carcinoma in Japan based on a newly established guideline managed by Japanese Society of Thyroid Surgeons and Japanese Association of Endocrine Surgeons[J]. World J Surg, 2011, 35(1):111-121. doi: 10.1007/s00268-010-0832-6 [23] Uchino S, Noguchi S, Kawamoto H, et al. Familial nonmedullary thyroid carcinoma characterized by multifocality and a high recurrence rate in a large study population[J]. World J Surg, 2002, 26(8): 897-902. doi: 10.1007/s00268-002-6615-y [24] Hillenbrand A, Varhaug JE, Brauckhoff M, et al. Familial nonmedullary thyroid carcinoma-clinical relevance and prognosis: a European multicenter study, ESES Vienna presentation[J]. Langenbeck's Arch Surg, 2010, 395(7):851-858. doi: 10.1007/s00423-010-0696-0 [25] Capezzone M, Marchisotta S, Cantara S, et al. Familial non-medullary thyroid carcinoma displays the features of clinical anticipation suggestive of a distinct biological entity[J]. Endocr Relat Cancer, 2008, 15(4):1075-1081. doi: 10.1677/ERC-08-0080 [26] Fallah M, Pukkala E, Tryggvadottir L, et al. Risk of thyroid cancer in first-degree relatives of patients with non-medullary thyroid cancer by histology type and age at diagnosis: a joint study from five Nordic countries[J]. J Medi Gene, 2013, 50(6):373-382. doi: 10.1136/jmedgenet-2012-101412 [27] Canzian F, Amati P, Harach HR, et al. A gene predisposing to familial thyroid tumors with cell oxyphilia maps to chromosome 19p13.2 [J]. Am J Hum Genet, 1998, 63(6):1743-1748. doi: 10.1086/302164 [28] Malchoff CD, Sarfarazi M, Tendler B, et al. Papillary thyroid carcinoma associated with papillary renal neoplasia: genetic linkage analysis of a distinct heritable tumor syndrome[J]. J Clin Endocrinol Metab, 2000, 85(5):1758-1764. doi: 10.1210/jcem.85.5.6557 [29] Bevan S, Pal T, Greenberg CR, et al. A comprehensive analysis of MNG1, TCO1, fPTC, PTEN, TSHR, and TRKA in familial nonmedullary thyroid cancer: confirmation of linkage to TCO1[J]. J Clin Endocrinol Metab, 2001, 86(8):3701-3704. doi: 10.1210/jcem.86.8.7725 [30] 董莉, 于洋, 于津浦, 等.二代测序技术应用于家族性非髓样甲状腺癌易感基因筛查[J].中华肿瘤杂志, 2017, 39(1):24-28. http://cdmd.cnki.com.cn/Article/CDMD-10062-1016924049.htmDong L, Yu Y, Yu JP, et al. Next generation sequencing technology for susceptible gene screening in familial non-medullary thyroid carcinoma[J]. Chin J Oncol, 2017, 39(1):24-28. http://cdmd.cnki.com.cn/Article/CDMD-10062-1016924049.htm -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 83
- HTML全文浏览量: 18
- PDF下载量: 1
- 被引次数: 0
