
Treatment of hypermyoglobinemia after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for patients with peritoneal carcinomatosis: a cohort study on 60 patients
-
摘要:
目的 探讨腹膜癌患者接受肿瘤细胞减灭(cytoreductive surgery,CRS)联合腹腔热灌注化疗(hyperthermic intraperitoneal chemotherapy,HIPEC)术后血肌红蛋白(myoglobin,Mb)水平的变化及其临床意义。 方法 回顾性研究60例接受CRS+HIPEC的腹膜癌病例。患者术后均出现高肌红蛋白血症,给予碳酸氢钠静脉输注及补液治疗。测定手术前后Mb、尿素氮、肌酐的浓度变化。 结果 CRS+HIPEC术后Mb水平明显升高,手术当日即达到高峰(416.667±110.966)μg/L。静脉输注碳酸氢钠有助于降低Mb水平及潜在风险。Mb水平在术后3~4d下降至正常范围内。血尿素氮(BUN)水平在术后升高,在术后第4天达峰值。血钙(Cr)在术后2天开始下降。1例患者发展为肾功能不全,脓毒血症,术后第26天死亡。其他患者均恢复良好。 结论 CRS+HIPEC术后常出现高肌红蛋白血症,Mb是内环境不稳定的一个早期而敏感指标。静脉输注碳酸氢钠可迅速降低Mb水平,减轻主要脏器功能损害。 Abstract:Objective For cancer patients who underwent extensive surgery, drastic release of myoglobin (Mb) after surgery can cause hypermyoglobinemia and related problems. This retrospective cohort study aims to summarize our experience and outcomes of 60 patients with hypermyoglobinemia after cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC), to investigate the changes in postoperative Mb levels, and to explore the clinical value of Mb. Methods This retrospective study covered 60 patients with peritoneal carcinomatosis who were treated with CRS and HIPEC. All patients developed hypermyoglobinemia after operation. Immediately after CRS and HIPEC, the patients were placed in a comprehensive treatment regimen consisting of hemodynamic stabilization therapies, nutritional support, anti-sepsis therapies, and psycho-physical therapies. For the treatment of hypermyoglobinemia, intravenous injection of sodium bicarbonate solution according to the Mb level was given to the patients. Moreover, the preand post-operative concentrations of Mb, blood urea nitrogen (BUN), and creatinine (Cr) were evaluated. Results Serum Mb levels after CRS and HIPEC were significantly elevated and peaked on the surgery day. Prompt treatment with intravenous infusion of sodium bicarbonate solution could help decrease the serum Mb levels and alleviate potential damage. Serum Mb levels returned to normal in approximately 3-4 days. The serum BUN levels increased after operation and peaked on the fourth postoperative day. On the other hand, serum Cr levels increased 2 days after operation and began to decrease on the third postoperative day. One patient developed renal failure and sepsis and died on postoperative day 26. The other patients recovered from the surgery without major adverse events. Conclusion Hypermyoglobinemia is a common lab abnormality after CRS and HIPEC, and serum Mb levels could be an early and sensitive indicator for dramatic disturbances in the internal milieu after surgery. Adequate treatment with sodium bicarbonate could accelerate the reduction in serum Mb levels and reduce the risk for major organ damages. -

图 1 血清Mb水平变化
Figure 1. Variation of serum Mb levels
Mb-1: Serum Mb levels before surgery; Mb0: Serum Mb levels at 0th day after surgery; Mb1: Serum Mb levels at 1st day after surgery; Mb2: Serum Mb levels at 2nd day after surgery; Mb3: Serum Mb levels at 3rd day after surgery; Mb4: Serum Mb levels at 4th day after surgery. Unit of Mb: mg/L. Normal range: male (17.4-105.7 μg/L); female (14.3-65.8 μg/L)

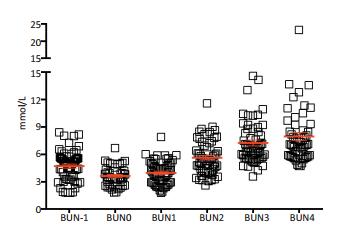
图 2 血清BUN水平变化
Figure 2. Variation of serum BUN levels
BUN-1: Serum BUN levels before surgery; BUN0: Serum BUN levels at 0th day after surgery; BUN1: Serum BUN levels at 1st day after surgery; BUN2: Serum BUN levels at 2nd day after surgery; BUN3: Serum BUN levels at 3rd day after surgery; BUN4: Serum BUN levels at 4th day after surgery. Unit of BUN: mmol/L. Normal range: 2.10-7.90 mmol/L

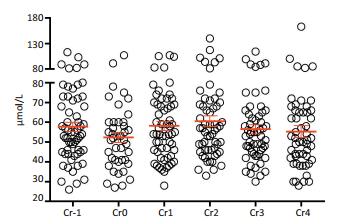
图 3 血清Cr水平变化
Figure 3. Variation of serum Cr levels
Cr-1: Serum Cr levels before surgery; Cr0: Serum Cr levels at 0th day after surgery; Cr1: Serum Cr levels at 1st day after surgery; Cr2: Serum Cr levels at 2nd day after surgery; Cr3: Serum Cr levels at 3rd day after surgery; Cr4: Serum Cr levels at 4th day after surgery. Unit of Cr: μmol/L. Normal range: 35-80 μmol/L
表 1 60例患者主要临床病理特征
Table 1. Major clinicopathologic characteristics of the 60 patients

-
[1] Li Y, Zhou YF, Liang H, et al. Chinese expert consensus on cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal malignancies[J]. World J Gastroenterol, 2016, 22(30):6906-6916. doi: 10.3748/wjg.v22.i30.6906 [2] Chua TC, Moran BJ, Sugarbaker PH, et al. Early-and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy[J]. J Clin Oncol, 2012, 30(20):2449-2456. doi: 10.1200/JCO.2011.39.7166 [3] Verwaal VJ, Van Ruth S, De Bree E, et al. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer[J]. J Clin Oncol, 2003, 21(20):3737-3743. doi: 10.1200/JCO.2003.04.187 [4] Sun JH, Ji ZH, Yu Y, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy to treat advanced/recurrent epithelial ovarian cancer: results from a retrospective study on prospectively established database[J]. Transl Oncol, 2016, 9(2):130-138. doi: 10.1016/j.tranon.2016.02.002 [5] Spiliotis J, Halkia E, Lianos E, et al. Cytoreductive surgery and HIPEC in recurrent epithelial ovarian cancer: a prospective randomized phase Ⅲ study[J]. Ann Surg Oncol, 2015, 22(5):1570-1575. doi: 10.1245/s10434-014-4157-9 [6] Yang XJ, Huang CQ, Suo T, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: final results of a phase Ⅲ randomized clinical trial[J]. Ann Surg Oncol, 2011, 18(6):1575-1581. doi: 10.1245/s10434-011-1631-5 [7] Sun JH, Ji ZH, Peng KW, et al. Cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy for the treatment of primary peritoneal serous carcinoma: Results of a Chinese retrospective study[J]. Int J Hyperthermia, 2016, 32(3):289-297. doi: 10.3109/02656736.2016.1146802 [8] Yao L, Liu Z, Zhu J, et al. Higher serum level of myoglobin could predict more severity and poor outcome for patients with sepsis[J].Am J Emerg Med, 2016, 34(6):948-952. doi: 10.1016/j.ajem.2016.01.009 [9] Premru V, Kovac J, Ponikvar R. Use of myoglobin as a marker and predictor in myoglobinuric acute kidney injury[J]. Ther Apher Dial, 2013, 17(4):391-395. doi: 10.1111/tap.2013.17.issue-4 [10] Sloventantor V, Poluektova MV, Poverennyi AM, et al. Postoperative hypermyoglobinemia. Mechanism of occurrence. Predictive[J]. Vopr Med Khim, 1995, 41(2):45-49. https://www.ncbi.nlm.nih.gov/pubmed/7793097 [11] Wu HT, Peng KW, Ji ZH, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy with lobaplatin and docetaxel to treat synchronous peritoneal carcinomatosis from gastric cancer: results from a Chinese center[J]. Eur J Surg Oncol, 2016, 42(7):1024-1034. [12] Huang CQ, Feng JP, Yang XJ, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from colorectal cancer: a case-control study from a Chinese center[J]. J Surg Oncol, 2014, 109(7):730-739. doi: 10.1002/jso.23545 [13] Huang CQ, Yang XJ, Yu Y, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy improves survival for patients with peritoneal carcinomatosis from colorectal cancer: a phase Ⅱ study from a Chinese center[J]. PLoS One, 2014, 9(9):e108509. doi: 10.1371/journal.pone.0108509 [14] Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis [J].Cancer Treat Res, 1996, 82:359-374. doi: 10.1007/978-1-4613-1247-5 [15] Sugarbaker PH. Peritonectomy procedures[J]. Ann Surg, 1995, 221(1):29-42. doi: 10.1097/00000658-199501000-00004 [16] Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative approach to pseudomyxoma peritonei syndrome[J]. Eur J Surg Oncol, 2001, 27(3):239-243. doi: 10.1053/ejso.2000.1038 [17] Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury[J]. N Engl J Med, 2009, 361(1):62-72. doi: 10.1056/NEJMra0801327 [18] Zhang XM, Tang Y, Yang YY, et al. Preliminary study on the pathogenic mechanism of myoglobin-induced endoplasmic reticulum stress and apoptosis in crush syndrome[J]. Sichuan Da Xue Xue Bao Yi Xue Ban, 2015, 46(1):22-26. https://www.ncbi.nlm.nih.gov/pubmed/25807790 [19] Poluektova MV, Sloventantor V, Khmelevskii Ia M, et al. Dynamics of the level of plasma myoglobin in oncology patients with and without complications in the postoperative period[J]. Vopr Med Khim, 1995, 41(1):47-49. doi: 10.1056/NEJM197410172911601 [20] Schneider AG, Bellomo R, Reade M, et al. Safety evaluation of a trial of lipocalin-directed sodium bicarbonate infusion for renal protection in at-risk critically ill patients[J]. Crit Care Resusc, 2013, 15(2):126-133. https://www.ncbi.nlm.nih.gov/pubmed/23931044 -

 下载:
下载:
 点击查看大图
点击查看大图

计量
- 文章访问数: 72
- HTML全文浏览量: 23
- PDF下载量: 2
- 被引次数: 0
