
-
摘要:
目的 探讨磁共振成像(magnetic resonance imaging,MRI)引导下微钻钻孔立体定向活检术在颅内占位性病变的应用。 方法 回顾性分析2009年11月至2013年12月就诊于首都医科大学三博脑科医院103例因脑幕上病变行MRI引导微钻钻孔立体定向活检手术的患者,分析病变的病理结果及患者术后情况。 结果 102例患者均获取明确的病理诊断,活检阳性率99.0%,其中胶质瘤66例(65.0%),淋巴瘤27例(26.5%),横纹肌肉瘤1例(1.0%),生殖细胞肿瘤3例(2.9%),炎性病变3例(2.9%),脑灰质异位2例(2.0%),脑梗塞1例(1.0%)。3例患者术后出现穿刺部位出血(2.9%),1例(1.0%)需行手术清除血肿,无死亡病例,无术后感染病例。 结论 磁共振引导微钻钻孔脑立体定向活检术是一种安全、可靠、微创的手术方法,对颅内病变的诊断与治疗具有重要意义。 Abstract:Objective To evaluate the reliability and accuracy of MRI-guided stereotactic biopsy for supratentorial brain lesions. Method A total of 103 cases of MRI-guided biopsy were performed between November 2009 and December 2013. Patients' pathological results and postoperative rehabilitation courses were analyzed. Results A total of 102 patients (99.0%) had pathological results, of which 97 cases were brain tumors (86.0%), including 36 cases of astrocytoma, 9 cases of anaplastic astrocytoma, 10 cases of oligoastrocytoma, 4 cases of anaplastic oligoastrocytoma, 4 cases of anaplastic oligodendroglioma, 3 cases of glioblastoma multiforme, 27 cases of lymphoma, 3 cases of germ cell tumors, and 1 case of rhabdomyosarcoma. Inflammatory lesions were found in 3 cases (2.9%). Displacement of brain gray matter was reported in 2 cases (2.0%), and 1 case (1.0%) of cerebral infarction existed. A total of 3 patients suffered intracranial hematoma after biopsy, and 1 patient underwent craniotomy to remove the hematoma. No death or intracranial inflammation occurred after biopsy. Conclusion MRI-guided stereotactic biopsy is a safe and reliable method in qualitative diagnosis. It is a very important tool for diagnosis and treatment selection for intracranial lesions. -
Key words:
- stereotactic techniques /
- brain diseases /
- biopsy /
- magnetic resonance imaging
-

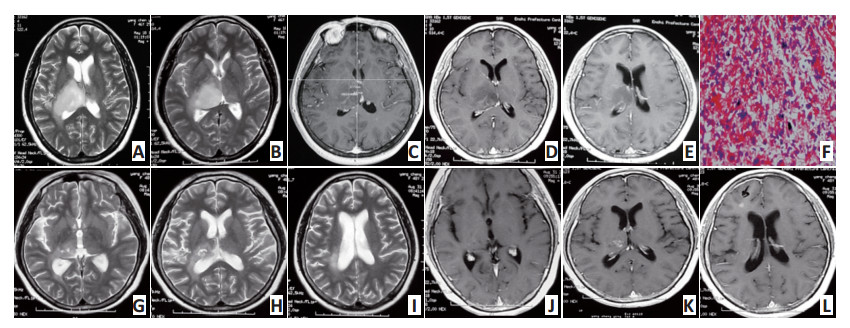
图 1 患者女,56岁,因左偏身麻木1月入院。检查结果示原发中枢神经系统淋巴瘤,患者术后行系统化疗
Figure 1. A 56-year old female, with left side numbess for 1 month. Imaging examination showed primary central nervous system lymphoma. The patient received postoperative chemotherapy
A and B.Preoperative MR flair image; C and D. Preoperative enhancing image; E and F. Preoperative CT image; G: Biopsy image; H. Pathological section (H&E staining, ×100 magnification) showed of non-Hodgkin's and diffuse large B-cell lymphoma

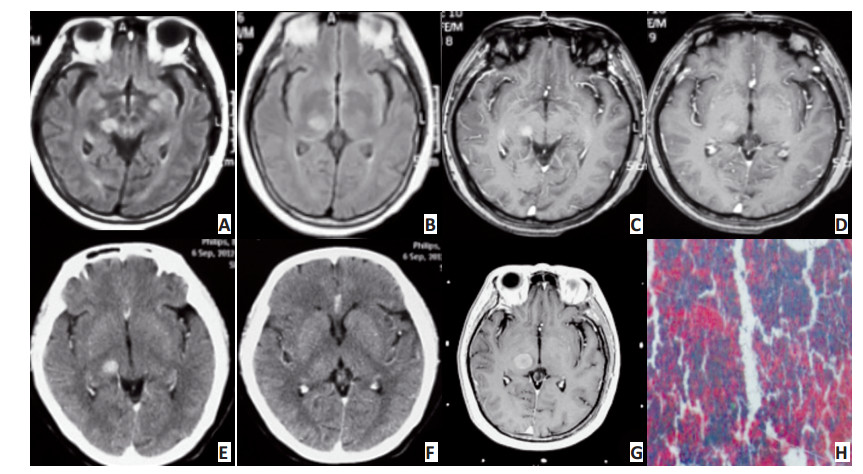
图 2 患者女,47岁,因左下肢乏力2个月入院。经治疗13个月后,MRI示肿瘤明显缩小
Figure 2. A 47-year old female patient was admitted to the hospital because of the left leg weakness for 2 months. She received sequential therapy for 13 months, and MRI showed the tumor significantly shrinked
A and B. Preoperative MR T2 image showed right thalamus lesion with high signal; C. Biopsy image; D and E. Preoperative enhancement image showed no enhancing; F. Pathological section (H&E staining, ×200 magnification) showed of anaplastic astrocytoma; G, H, and I. Postoperative T2 imaging results at 13 months after brain biopsy treatment followed by local radiotherapy and chemotherapy; J, K, and L. Postoperative enhancing MR images after 13 months, showing that the tumor significantly shrinked and the disease controlled well
-
[1] Hall WA. The safety and efficacy of stereotactic biopsy for intracranial lesions[J]. Cancer, 1998, 82(9):1749-1755. doi: 10.1002/(ISSN)1097-0142 [2] 刘宗惠, 陈琳, 于新, 等.805例立体定向脑活检报告[J].中国神经精神疾病杂志, 2004, 30(6):401-404. http://www.cnki.com.cn/Article/CJFDTOTAL-ZSJJ200406000.htmLiu ZH, Chen L, Yu, X, et al. Stereotactic biopsy for the brain lesions:experience of 805 cases[J]. Chin J Nervous Mental Dis, 2004, 30(6):401-404. http://www.cnki.com.cn/Article/CJFDTOTAL-ZSJJ200406000.htm [3] 刘宗惠, 于新, 李士月, 等.脑深部病变立体定向活检方法的研究[J].中华医学杂志, 2002, 82(04):225-228. doi: 10.3760/j:issn:0376-2491.2002.04.004Liu ZH, Yu X, Li SY, et al. Stereotactic biopsy for intracranial deep lesions[J]. Natl Medi J China, 2002, 82(04):225-228. doi: 10.3760/j:issn:0376-2491.2002.04.004 [4] Dammers R, Schouten JW, Haitsma IK, et al. Towards improving the safety and diagnostic yield of stereotactic biopsy in a single centre[J]. Acta Neurochirurgica, 2010, 152(11):1915-21. doi: 10.1007/s00701-010-0752-0 [5] 曹国彬, 柯炎斌, 何伟文, 等.原发K性颅内淋巴瘤的临床特点及其治疗探讨[J].广东医学, 2009, 30(7):1120-1121.Cao GB, Ke YB, He WW, et al. Clinical features and treatment of primary intracranial lymphoma[J]. Guangdong Medi J, 2009, 30(7):1120-1121. [6] 张剑宁, 程岗, 王亚明, 等.立体定向活检诊断原发性中枢神经系统淋巴瘤(118例临床及影像学特征)[J].立体定向和功能性神经外科杂志, 2012, 25(03):129-133. http://www.cnki.com.cn/Article/CJFDTOTAL-NENG201203002.htmZhang JN, Cheng G, Wang YM, et al. Stereotactic biopsy in the diagnosis of primary central nervous system lymphoma(clinical and imaging features of 118 cases)[J]. Chin J Stereot Funct Neuro, 2012, 25(3):129-133. http://www.cnki.com.cn/Article/CJFDTOTAL-NENG201203002.htm [7] 廖声潮, 黄玮杨, 雷霆, 等.立体定向活检诊断脑低级别星形细胞瘤[J].中华外科杂志, 2009, 47(1):71-72. http://cdmd.cnki.com.cn/Article/CDMD-10183-2008061856.htmLiao SC, Huan WY, Lei T, et al. Stereotactic biopsy in the diagnosis of low grade astrocytoma[J]. Chin J Surg, 2009, 47(1):71-72. http://cdmd.cnki.com.cn/Article/CDMD-10183-2008061856.htm [8] 玉石, 王亚明, 李春森, 等.立体定向活检在MRI表现不典型的多形性胶质母细胞瘤中的应用[J].中国微侵袭神经外科杂志, 2013, 18(5):227-228. doi: 10.11850/j.issn.1009-122X.2013.05.013Yu S, Wang YM, Li CS, et al. Application of stereotactic biopsy in the atypical MRI of polymorphic glioblastoma[J]. Chin J Minimal Inv Neuro, 2013, 18(5):227-228. doi: 10.11850/j.issn.1009-122X.2013.05.013 [9] Ng WH, Lim T. Targeting regions with highest lipid content on MR spectroscopy may improve diagnostic yield in stereotactic biopsy[J].J Clin Neuro Offic J Neuro Soci Australasia, 2008, 15(05):502-506. doi: 10.1007/s11060-011-0601-x [10] 田增民, 王亚明, 于新, 等.立体定向脑内病灶活检的临床意义[J].中华外科杂志, 2010, 48(19):1459-1462. doi: 10.3760/cma.j.issn.0529-5815.2010.19.006Tian ZM, WANG YM, Yu X, et al. Clinical experience of stereotactic biopsy for the brain lesions[J]. Chin J Surg, 2010, 48(19):1459-1462. doi: 10.3760/cma.j.issn.0529-5815.2010.19.006 [11] Abdelaziz O, Eshra M, Belal A, et al. Diagnostic value of magnetic resonance spectroscopy compared with stereotactic biopsy of Intra-axial brain lesions[J]. J Neuro Sur Part A Central European Neurosurgery, 2016, 77(04):283-290. doi: 10.1055/s-00000180 [12] Capitanio JF, Camporesi S, Franzin A, et al. Inverted positioning ofLeksell Frame G for very low posterior fossa and brain stem lesions biopsies[J]. J Neuro Sci, 2016 -

 下载:
下载:
 点击查看大图
点击查看大图
计量
- 文章访问数: 51
- HTML全文浏览量: 26
- PDF下载量: 0
- 被引次数: 0
