
The effect of different excision methods on the prognosis of type Ⅲ and Ⅳ hilar cholangiocarcinoma
-
摘要:
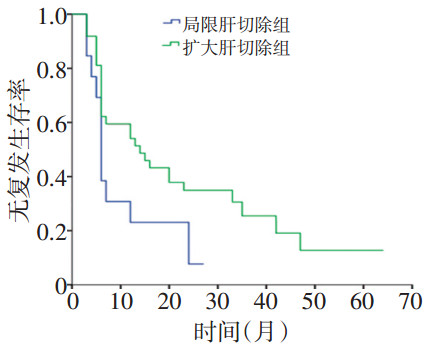
目的 比较Ⅲ、Ⅳ型肝门胆管癌(hilar cholangiocarcinoma,HC)手术治疗方式及疗效。 方法 回顾性分析自2010年1月至2015年12月就诊于天津医科大学肿瘤医院行手术治疗的50例Ⅲ、Ⅳ型HC患者的临床资料。 结果 50例HC患者获得随访,中位随访时间为27个月。其中围肝门局限肝切除组13例,中位无复发时间为6个月,1、2年无复发率分别为30.8%、23.1%;中位生存时间为20个月,1、2年生存率分别为76.9%、38.5%;扩大肝切除组37例,中位无复发时间为14个月,1、2年无复发率分别为59.5%、32.4%;中位生存时间为37个月,1、2年生存率分别为83.8%、51.4%。扩大肝切除组无复发时间及生存时间均长于围肝门局限肝切除组(P<0.05),1、2年无复发生存率及总生存率也更高(P<0.05),但是两组并发症发生率及病死率并无显著差异(P>0.05)。 结论 扩大肝切除术是延缓Ⅲ、Ⅳ型HC患者早期复发、改善生存预后的安全术式。 Abstract:Objective To compare the relationship between the operative strategies and clinical outcomes of type Ⅲ and Ⅳ hilar cholangiocarcinomas (HCs). Methods We retrospectively analyzed the clinical data and long-term outcomes for 50 cases of type Ⅲ and Ⅳ HC that underwent surgery at the Tianjin Medical University Cancer Hospital. Results Fifty patients were followed up and the median follow-up duration was 27 months. The hilar limited hepatectomy group included 13 cases; the median disease-free survival was 6 months, and 1-and 2-year disease-free survival rates were 30.8% and 23.1%, respectively. The median overall survival was 20 months, and the 1-and 2-year overall survival rates were 76.9% and 38.5%, respectively. The extended hepatectomy group included 37 cases; the median disease-free survival was 14 months, and 1-and 2-year disease-free survival rates were 59.5% and 32.4%, respectively. The median overall survival was 37 months, and the 1-and 2-year overall survival rates were 83.8% and 51.4%, respectively. Compared with the hilar limited hepatectomy group, the extended hepatectomy group had significantly longer median disease-free and overall survival (P < 0.05). The 1-and 2-year disease-free and overall survival rates were higher for the extended hepatectomy group. There was no significant difference in morbidity and mortality between the two groups (P > 0.05). Conclusions Extended hepatectomy is a safe operation that delays recurrence at early time points and improves the prognosis for patients with typeⅢand ⅣHC. -
Key words:
- cholangiocarcinoma hepatectomy /
- resection rate /
- postoperative complications /
- prognosis
-
表 1 两组患者术前情况 n(%)

表 2 两组患者术中情况、术后并发症及恢复情况 n(%)

表 3 两组患者病理及辅助治疗 n(%)

-
[1] Saxena A, Chua TC, Chu FC, et al. Improved outcomes after aggressive surgical resection of hilar cholangiocarcinoma: a critical analysis of recurrence and survival[J]. Am J Surg, 2011, 202(3):310-320. doi: 10.1016/j.amjsurg.2010.08.041 [2] Launois B, Reding R, Lebeau G, et al. Surgery for hilar cholangiocarcinoma: French experience in a collective survey of 552 extrahepatic bile duct cancers[J]. J Hepatobiliary Pancreat Surg, 2000, 7(2):128-134. doi: 10.1007/s005340050166 [3] Dinant S, Gerhards MF, Rauws EA, et al. Improved outcome of resection of hilar cholangiocarcinoma (Klatskin tumor)[J]. Ann Surg Oncol, 2006, 13(6):872-880. doi: 10.1245/ASO.2006.05.053 [4] Lillemoe KD, Cameron JL. Surgery for hilar cholangiocarcinoma:the Johns Hopkins approach[J]. J Hepatobiliary Pancreat Surg, 2000, 7 (2):115-121. doi: 10.1007/s005340050164 [5] Young AL, Prasad KR, Toogood GJ, et al. Surgical treatment of hilar cholangiocarcinoma in a new era:comparison among leading Eastern and Western centers, Leeds[J]. J Hepatobiliary Pancreat Sci, 2010, 17(4):497-504. doi: 10.1007/s00534-009-0203-6 [6] Ercolani G, Zanello M, Grazi GL, et al. Changes in the surgical approach to hilar cholangiocarcinoma during an 18-year period in a Western single center[J]. J Hepatobiliary Pancreat Sci, 2010, 17(3): 329-337. doi: 10.1007/s00534-009-0249-5 [7] Lee SG, Song GW, Hwang S, et al. Surgical treatment of hilar cholangiocarcinoma in the new era:the Asan experience[J]. J Hepatobiliary Pancreat Sci, 2010, 17(4):476-489. doi: 10.1007/s00534-009-0204-5 [8] 陈孝平, 黄志勇, 陈义发, 等.肝门部胆管癌根治术肝切除范围的合理选择[J].中国普通外科杂志, 2013, 22(1):8-9. http://d.wanfangdata.com.cn/Periodical_zgptwkzz201301003.aspx [9] Chen XP, Lau WY, Huang ZY, et al. Extent of liver resection for hilar cholangiocarcinoma[J]. Br J Surg, 2009, 96(10):1167-1175. doi: 10.1002/bjs.v96:10 [10] Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM[J]. Ann Surg Oncol, 2010, 17(6):1471-1474. doi: 10.1245/s10434-010-0985-4 [11] Benson AR, Abrams TA, Ben-Josef E, et al. NCCN clinical practice guidelines in oncology:hepatobiliary cancers[J]. J Natl Compr Canc Netw, 2009, 7(4):350-391. doi: 10.6004/jnccn.2009.0027 [12] 黄志强.肝门部胆管癌的外科治疗与发展[J].中国普外基础与临床杂志, 2003, 10(5):425-428. http://d.old.wanfangdata.com.cn/Periodical/zgpwjcylczz200305001 [13] Nanashima A, T obinaga S, Abo T, et al. Left hepatectomy accompanied by a resection of the whole caudate lobe using the dorsally fixed liver-hanging maneuver[J]. Surg Today, 2011, 41(3):453-458. doi: 10.1007/s00595-010-4291-3 [14] Jarnagin WR, Fong Y, DeMatteo RP, et al. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma[J]. Ann Surg, 2001, 234(4):507-17. doi: 10.1097/00000658-200110000-00010 [15] Nishio H, Hidalgo E, Hamady ZZ, et al. Left hepatic trisectionectomy for hepatobiliary malignancy: results and an appraisal of its current role[J]. Ann Surg, 2005, 242(2):267-75. doi: 10.1097/01.sla.0000171304.70678.11 [16] 陈孝平, 黄志勇, 张志伟, 等.小范围肝切除治疗Bismuth-Corlette Ⅲ型肝门部胆管癌[J].中华外科杂志, 2009, 47(15):1148-1150. doi: 10.3760/cma.j.issn.0529-5815.2009.15.010 [17] 周宁新, 黄志强, 张文智, 等.402例肝门部胆管癌临床分型、手术方式与远期疗效的综合分析[J].中华外科杂志, 2006, 44(23):1599-1603. doi: 10.3760/j:issn:0529-5815.2006.23.006 [18] van Gulik TM, Kloek JJ, Ruys AT, et al. Multidisciplinary management of hilar cholangiocaroma(Klatskin tumor):extended resection is associated with improved survival[J]. Eur J Surg Oncol, 2011, 37 (1):65-71. doi: 10.1016/j.ejso.2010.11.008 [19] Lee SG, Lee YJ, Park KM, et al. One hundred and eleven liver resections for hilar bile duct cancer[J]. J Hepatobiliary Pancreat Surg, 2000, 7(2): 135-141. doi: 10.1007/s005340050167 -

 下载:
下载:
 点击查看大图
点击查看大图

图(2) / 表(3)
计量
- 文章访问数: 104
- HTML全文浏览量: 11
- PDF下载量: 2
- 被引次数: 0
