
A clinical study of standard remnant liver volume in predicting post-hepatectomy liver failure in patients with hepatocellular carcinoma after hemihepatectomy of cirrhotic liver
-
摘要:
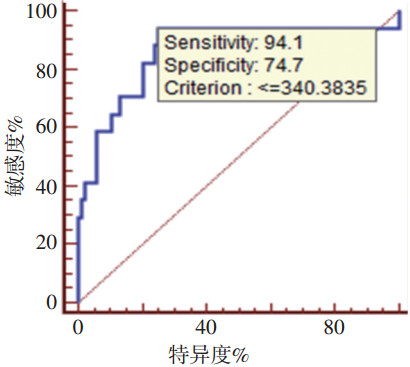
目的 探讨肝细胞癌(hepatocellular carcinoma,HCC)合并肝硬化患者肝切术标准残肝体积(the standard remnant liver vol-ume,SRLV)的安全临界值及其评估术后肝功能衰竭(post-hepatectomy liver failure,PHLF)的效能。 方法 回顾性分析广西医科大学附属肿瘤医院2013年9月~2016年8月共181例半肝切除术HCC患者临床资料,术前测定肝脏总体积、肿瘤体积、残肝体积、切除的肝体积。术中排水法测定切除标本的体积。按照“50-50标准”分成肝衰竭组(22例)与无肝衰竭组(159例),分析发生PHLF的相关因素,统计分析肝硬化亚组SRLV的临界值及其预测PHLF效能,并回顾性分析肝硬化患者的CT分级资料。 结果 术后共发生PHLF 22例,PHLF相关死亡1例。多因素分析显示术前胆红素水平及SRLV是发生PHLF的危险因素。按照肝硬化病理进行亚组分析,肝硬化组102例(Ⅰ、Ⅱ级肝硬化84例,Ⅲ级肝硬化18例,无Ⅳ级肝硬化),18例发生PHLF,PHLF相关死亡1例。HCC合并肝硬化行半肝切除发生PHLF的SRLV临界值为340 mL/m2(灵敏度94.4%,特异度74.7%,曲线下面积0.861,P<0.01)。 结论 SRLV≤340 mL/m2的HCC合并肝硬化患者在行半肝切除术后,发生PHLF的风险增高。 Abstract:Objective To explore the correlation between standard remnant liver volume (SRLV) and post-hepatectomy liver failure (PHLF) in patients with hepatocellular carcinoma (HCC) and cirrhotic livers. Methods In total, 181 patients who underwent hemihepatectomy in Affiliated Tumor Hospital of Guangxi Medical University from September 2013 to August 2016 were enrolled in the study. Total liver, tumor, remnant liver, and resected liver volumes were measured using the Myrian liver surgical planning system before surgery. Intraoperative resected liver volume (including resected normal liver and tumor volumes) were collected using the drainage method. The patients were divided into the PHLF (22 cases) and non-PHLF groups (159 cases) according to whether PHLF occurred based on the "50/50" criteria. The risk factors of PHLF were then explored. The cut-off of SRLV and efficiency of predicting PHLF were analyzed in the subgroup of patients with cirrhotic livers. The grade of liver cirrhosis was retrospectively analyzed using helical computed tomography (CT). Results Twenty-two of the 181 patients developed PHLF and one died of it. Preoperative total bilirubin levels and SRLV were identified as independent factors for predicting PHLF using a Logistic regression model. In total, 102 patients with cirrhotic livers were selected in subgroup analysis based on postoperative cirrhotic pathology. Eighteen patients developed PHLF and one died of PHLF in the subgroup. Using receiver-operating characteristic (ROC) curve analysis, 340 mL/m2 was the cut-off of SRLV for patients with HCC and cirrhotic livers (area under the curve: 0.861, P < 0.01; sensitivity and specialty rates were 94.4% and 74.7%, respectively). Eighty-four cases were of grade Ⅰ or Ⅱ cirrhosis, 18 cases were of grade Ⅲ cirrhosis, and there were no cases of grade Ⅳ cirrhosis based on retrospective analysis using helical CT. Conclusions Patients with cirrhotic livers with an anticipated SRLV of ≤340 mL/m2 after hepatic resection are at increased risk for PHLF after emihepatectomy. -
表 1 两组各项基线资料比较(x±s,n/n)

表 2 肝衰竭相关因素的logistic回归多因素分析

表 3 肝硬化程度CT分级 n(%)

-
[1] Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics[J]. CA Cancer J Clin, 2016, 66(4):271-289. doi: 10.3322/caac.v66.4 [2] Siegel RL, Miller KD, Jemal A. Cancer statistics[J]. CA Cancer J Clin, 2016, 66(1):7-30. doi: 10.3322/caac.21332 [3] Zhong JH, Ke Y, Gong WF, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma[J]. Ann Surg, 2014, 260(2): 329-340. doi: 10.1097/SLA.0000000000000236 [4] Rahbari NN, Garden OJ, Padbury R, et al. Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS)[J]. Surgery, 2011, 149(5):713-724. doi: 10.1016/j.surg.2010.10.001 [5] Jaeck D, Bachellier P, Oussoultzoglou E, et al. Surgical resection of hepatocellular carcinoma. Post-operative outcome and long-term results in Europe: an overview[J]. Liver Transpl, 2004, 10(2 Suppl 1): S58-63. http://europepmc.org/abstract/MED/14762841 [6] Paugam-Burtz C, Janny S, Delefosse D, et al. Prospective validation of the "fifty-fifty" criteria as an early and accurate predictor of death after liver resection in intensive care unit patients[J]. Ann Surg, 2009, 249(1):124-128. doi: 10.1097/SLA.0b013e31819279cd [7] Lafaro K, Buettner S, Maqsood H, et al. Defining Post Hepatectomy Liver Insufficiency: Where do We stand[J]. J Gastrointest Surg, 2015, 19(11):2079-2092. doi: 10.1007/s11605-015-2872-6 [8] Hyder O, Pulitano C, Firoozmand A, et al. A risk model to predict 90-day mortality among patients undergoing hepatic resection[J]. J Am Coll Surg, 2013, 216(6):1049-1056. doi: 10.1016/j.jamcollsurg.2013.01.004 [9] van den Broek MA, Olde Damink SW, Dejong CH, et al. Liver failure after partial hepatic resection: definition, pathophysiology, risk factors and treatment[J]. Liver Int, 2008, 28(6):767-780. doi: 10.1111/j.1478-3231.2008.01777.x [10] Abdalla EK, Barnett CC, Doherty D, et al. Extended hepatectomy in patients with hepatobiliary malignancies with and without preoperative portal vein embolization[J]. Arch Surg, 2002, 137(6):675-680. doi: 10.1001/archsurg.137.6.675 [11] Kishi Y, Abdalla EK, Chun YS, et al. Three hundred and one consecutive extended right hepatectomies: evaluation of outcome based on systematic liver volumetry[J]. Ann Surg, 2009, 250(4):540-548. http://europepmc.org/abstract/MED/19730239 [12] 朱化刚.术前肝脏储备功能的判断与安全肝切除量[J].肝胆外科杂志, 2005, 13(16):406-409. http://d.old.wanfangdata.com.cn/Periodical/gdwkzz200506003 [13] Shirabe K, Shimada M, Gion T, et al. Postoperative liver failure after major hepatic resection for hepatocellular carcinoma in the modern era with special reference to remnant liver volume[J]. J Am Coll Surg, 1999, 188(3):304-309. doi: 10.1016/S1072-7515(98)00301-9 [14] Balzan S, Belghiti J, Farges O, et al. The "50-50 criteria" on postoperative day 5: an accurate predictor of liver failure and death after hepatectomy[J]. Ann Surg, 2005, 242(6):824-828. doi: 10.1097/01.sla.0000189131.90876.9e [15] 中华医学会传染病与寄生虫病学分会.病毒性肝炎防治方案[J].中华肝脏病杂志, 2000, 8(6):324-329. http://d.wanfangdata.com.cn/Periodical_zhcrbzz200101027.aspx [16] 宇传华, 徐勇勇, 夏结来, 等.人体表面积的计算公式[J].中华预防医学杂志, 1999, 33(32):123-124. http://www.doc88.com/p-2896718021854.html [17] 涂蓉, 伍保忠, 郑妙琼.肝硬化CT分级方法研究[J].放射学实践, 2003, 18(9):2621-2623. http://www.cqvip.com/QK/94342X/200309/9013969.html [18] Steger U, Kellersmann A, Germer CT. Hemihepatectomy[J]. Zentralbl Chir, 2016, 141(3):253-255. doi: 10.1055/s-00000104 [19] 陈熙, 杜正贵, 李波, 等.标准残肝体积对肝脏储备功能的评价[J].世界华人消化杂志, 2010, 18(17):1829-1833. doi: 10.3969/j.issn.1009-3079.2010.17.016 [20] 龚文锋, 张志远, 陆战, 等.乙肝病毒相关性肝癌术后标准残肝体积及其与术后肝功能代偿不全关系的研究[J].广西医学, 2015, 37 (39):1226-1230. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=gxyx201509006 [21] 孙惠川, 汤敏, 钦伦秀, 等.用余肝体积预测半肝切除耐受性的安全标准[J].中华肝胆外科杂志, 2006, 12(16):366-369. http://med.wanfangdata.com.cn/Paper/Detail/PeriodicalPaper_zhgdwk200606004 -

 下载:
下载:
 点击查看大图
点击查看大图
图(1) / 表(3)
计量
- 文章访问数: 44
- HTML全文浏览量: 4
- PDF下载量: 1
- 被引次数: 0
