
The clinical value of predicting the invasiveness of pulmonary mixed ground-glass nodules by CT quantitative parameters
-
摘要:
目的 探讨CT定量参数对肺混合磨玻璃结节侵袭性的预测价值。 方法 回顾性分析天津医科大学肿瘤医院2013年1月至2016年9月经手术病理证实的164例肺混合磨玻璃结节(mixed ground glass nodules,mGGNs)患者的CT图像。利用受试者工作曲线(ROC)及Logistic回归分析法评估微浸润腺癌(minimally invasive adenocarcinoma,MIA)和浸润性腺癌(invasive adenocarcinoma,IAC)的CT定量参数(肺窗最大径、肺窗最大径的最大垂直径、肺窗病灶体积、平均CT值、纵隔窗最大径、纵隔窗最大径的最大垂直径、纵隔窗病灶体积以及肿瘤影消失率(tumor disappearance rate,TDR)差异。 结果 Logistic回归分析显示病灶肺窗最大径(OR=3.080,95%CI:1.135~8.355,P=0.027)及纵隔窗最大径(OR=5.881,95%CI:1.634~21.166,P=0.007)可独立预测mGGNs的侵袭性;两者联合应用所对应的曲线下面积为0.855,灵敏度为77.61%,特异度为86.67%,其截断点对应的肺窗最大径和纵隔窗最大径分别为1.902 cm和1.273 cm。 结论 CT定量参数有助于预测评估肺混合磨玻璃结节的侵袭性,病灶肺窗最大径及纵隔窗最大径是其独立预测因子。 Abstract:Objective To discuss the value of CT quantitative parameters in prediction of the invasiveness of pulmonary mixed ground glass nodules (mGGNs). Methods CT images of 164 patients with pulmonary ground-glass nodules (mGGNs), enrolled in Tianjin Medical University Cancer Institute and Hospital from January 2013 to September 2016, confirmed by surgical pathology were analyzed retrospectively. CT quantitative parameters including maximum diameter, largest diameter perpendicular to the maximum diameter, volume on both pulmonary window and mediastinal window, mean CT value and TDR (tumor shadow disappear rate) were evaluated between minimally invasive adenocarcinoma (MIA) and invasive adenocarcinoma (IAC) with ROC and Logistic regression analysis. Results Logistic regression analysis showed that the maximum diameter of the pulmonary window (OR=3.080, 95% CI:1.135-8.355, P= 0.027) and the maximum diameter of the mediastinal window (OR=5.881, 95%CI:1.634-21.166, P=0.007) independently predicted the invasiveness of mGGNs; the corresponding values of area under the curve of the combination of two parameters were 0.855, with sensitivity of 77.61% and specificity of 86.67 %. The cut-off point to the corresponding value of the maximum diameter on pulmonary window and mediastinal window was 1.902cm and 1.273cm, respectively. Conclusions CT quantitative parameters are helpful in predicting the invasiveness of mGGNs. The maximum diameters on both pulmonary window and mediastinal window are independent predictors. -
Key words:
- lung adenocarcinoma /
- mixed ground-glass nodules /
- invasiveness /
- CT /
- quantitative parameters
-

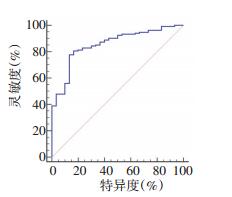
图 2 肺窗最大径联合纵隔窗最大径的ROC曲线
曲线下面积(AUC)为0.855(95%CI:0.786~0.923,P < 0.001),灵敏度为77.61%,特异度为86.67%
表 1 164例mGGNs的分类情况

表 2 两组中CT定量参数的分析

表 3 各参数的ROC曲线分析

表 4 ROC曲线成对比较有差异的参数

-
[1] Oh JY, Kwon SY, Yoon HI, et al. Clinical significance of a solitary ground-glass opacity (GGO) lesion of the lung detected by chest CT [J]. Lung Cancer, 2007, 55(1):67-73. doi: 10.1016/j.lungcan.2006.09.009 [2] Kim HY, Shim YM, Lee KSI, et al. Persistent pulmonary nodular ground-glass opacity at thin-section CT: histopathologic comparisons[J]. Radi, 2007, 245(1):267-275. doi: 10.1148/radiol.2451061682 [3] Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma[J]. J Thora Oncol, 2011, 6(2):244-285. doi: 10.1097/JTO.0b013e318206a221 [4] Dembitzer FR, Flores RM, Parides MK, et al. Impact of histologic subtyping on outcome in lobar vs sublobar resections for lung cancer: a pilot study[J]. Chest, 2014, 146(1):175-181. doi: 10.1378/chest.13-2506 [5] Yoshimoto K, Nomori H, Mori T, et al. Quantification of the impact of segmentectomy on pulmonary function by perfusion single-photon-emission computed tomography and multidetector computed tomography[J]. J Thora Cardi Surg, 2009, 137(5):1200-1205. doi: 10.1016/j.jtcvs.2008.10.028 [6] Macke RA, Schuchert MJ, Odell DD, et al. Parenchymal preserving anatomic resections result in less pulmonary function loss in patients with Stage Ⅰ non-small cell lung cancer[J]. J Thora Cardi Surg, 2015, (10):49. http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.793.864&rep=rep1&type=pdf [7] Yu Y, Jian H, Shen L, et al. Lymph node involvement influenced by lung adenocarcinoma subtypes in tumor size ≤3 cm disease: A study of 2268 cases[J]. Eur J Surg Oncol, 2016, 42(11):1714-1719. doi: 10.1016/j.ejso.2016.02.247 [8] Lee HJ, Goo JM, Lee CH, et al. Nodular ground-glass opacities on thin-section CT: size change during follow-up and pathological results[J]. Korean J Radi, 2007, 8(1):22-31. doi: 10.3348/kjr.2007.8.1.22 [9] Gao F, Ge XJ, Li M, et al. CT diagnosis of different pathological types of ground-glass nodules[J]. Chin J Oncol, 2014, 36(3):188-192. https://www.researchgate.net/publication/262016233_CT_diagnosis_of_different_pathological_types_of_ground-glass_nodules [10] Lee SM, Goo JM, Lee KH, et al. CT findings of minimally invasive adenocarcinoma (MIA) of the lung and comparison of solid portion measurement methods at CT in 52 patients[J]. Eur Radi, 2015, 25 (8):2318-2325. doi: 10.1007/s00330-015-3616-4 [11] Si MJ, Tao XF, Du GY, et al. Thin-section computed tomography-histopathologic comparisons of pulmonary focal interstitial fibrosis, atypical adenomatous hyperplasia, adenocarcinoma in situ, and minimally invasive adenocarcinoma with pure ground-glass opacity [J]. Eur J Radi, 2016, 85(10):1708-1715. doi: 10.1016/j.ejrad.2016.07.012 [12] Yanagawa M, Johkoh T, Noguchi M, et al. Radiological prediction of tumor invasiveness of lung adenocarcinoma on thin-section CT[J]. Med, 2017, 96(11):e6331. doi: 10.1097/MD.0000000000006331 [13] Zhang Y, Shen Y, Qiang JW, et al. HRCT features distinguishing preinvasive from invasive pulmonary adenocarcinomas appearing as ground-glass nodules[J]. Eur Radi, 2016, 26(9):2921-2928. doi: 10.1007/s00330-015-4131-3 [14] Son JY, Lee HY, Kim JH, et al. Quantitative CT analysis of pulmonary ground-glass opacity nodules for distinguishing invasive adenocarcinoma from non-invasive or minimally invasive adenocarcinoma: the added value of using iodine mapping[J]. Eur Radi, 2016, 26(1): 43-54. doi: 10.1007/s00330-015-3816-y [15] Kadota K, Villena-Vargas J, Yoshizawa A, et al. Prognostic significance of adenocarcinoma in situ, minimally invasive adenocarcinoma, and nonmucinous lepidic predominant invasive adenocarcinoma of the lung in patients with stage Ⅰ disease[J]. Am J Surg Path, 2014, 38(4):448-460. doi: 10.1097/PAS.0000000000000134 [16] Yanagawa M, Tanaka Y, Kusumoto M, et al. Automated assessment of malignant degree of small peripheral adenocarcinomas using volumetric CT data: correlation with pathologic prognostic factors[J]. Lung Cancer, 2010, 70(3):286-294. doi: 10.1016/j.lungcan.2010.03.009 [17] Ding H, Shi J, Zhou X, et al. Value of CT characteristics in predicting invasiveness of adenocarcinoma presented as pulmonary groundglass nodules[J]. Thoracic and cardiovascular surgeon, 2017, 65(2): 136-141. [18] Liu Y, Sun H, Zhou F, et al. Imaging features of TSCT predict the classification of pulmonary preinvasive lesion, minimally and invasive adenocarcinoma presented as ground glass nodules[J]. Lung Cancer, 2017, (108):192-197. https://www.sciencedirect.com/science/article/pii/S0169500217302660 [19] Eguchi T, Yoshizawa A, Kawakami S, et al. Tumor size and computed tomography attenuation of pulmonary pure ground-glass nodules are useful for predicting pathological invasiveness[J]. PloS One, 2014, 9(5):e97867. doi: 10.1371/journal.pone.0097867 [20] Matsuguma H, Oki I, Nakahara R, et al. Comparison of three measurements on computed tomography for the prediction of less in vasiveness in patients with clinical stage Ⅰ non-small cell lung cancer [J]. Ann Thora Surg, 2013, 95(6):1878-1884. doi: 10.1016/j.athoracsur.2013.02.022 [21] Takamochi K, Nagai K, Yoshida J, et al. Pathologic N0 status in pulmonary adenocarcinoma is predictable by combining serum carcinoembryonic antigen level and computed tomographic findings [J]. J Thora Cardiova Surg, 2001, 122(2):325-330. doi: 10.1067/mtc.2001.114355 -

 下载:
下载:
 点击查看大图
点击查看大图
图(2) / 表(4)
计量
- 文章访问数: 142
- HTML全文浏览量: 26
- PDF下载量: 2
- 被引次数: 0
