
Patterns of locoregional rectal cancer recurrences after total mesorectal excision and delineation of the radiotherapy clinical target volume
-
摘要:
目的 分析直肠癌全直肠系膜切除术(total mesorectal excision, TME)术后盆腔局部复发及转移规律, 为进一步细化直肠癌放疗靶区提供依据。 方法 回顾性分析2012年1月至2018年11月于重庆医科大学附属第一医院经影像学证实直肠癌TME术后有盆腔区域复发的134例患者临床资料, χ2检验分析患者原发肿瘤位置、术后分期等临床因素与淋巴结转移的相关性, 以及盆腔不同淋巴引流区之间转移的因果关系。 结果 134例患者中吻合口复发57例(42.5%), 直肠残端、术区及直肠周围复发36例(26.9%), 骶前淋巴引流区盆腔部复发34例(25.4%), 骶前淋巴引流区腹部复发10例(7.5%), 髂内淋巴引流区复发46例(34.3%), 髂外淋巴引流区复发5例(3.7%), 闭孔淋巴引流区复发0.7%(1/134), 腹股沟淋巴引流区复发13例(9.7%), 坐骨直肠窝复发11例(8.2%)。上段直肠癌较中下段直肠癌更易发生骶前淋巴引流区腹部转移(19.0% vs. 5.6%, P=0.028), 有腹股沟淋巴结转移的患者更易发生髂外淋巴引流区转移(23.1% vs. 1.7%, P=0.006)。 结论 上段及中下段直肠癌术后复发模式呈显著性差异, 放疗靶区应区别定义, 当前直肠癌靶区可进一步细化。 Abstract:Objective The characteristics of locoregional rectal cancer recurrences following total mesorectal excision (TME) were not clear previously. This study aimed to analyze and help determine the optimal radiotherapy clinical target volume. Methods The clinical data of 134 patients who had recurrence and metastasis following TME without radiotherapy between January 2012 and November 2018 in our hospital were retrospectively analyzed. The Chi-square test was used to evaluate the relationship between lymph node metastasis and clinicopathological factors, such as the location of primary tumors and tumor stage. The correlations between different types of lymphatic drainage of rectal cancer were also tested. Results In total, 134 patients were enrolled in this study. The median time to relapse was 15 months. The incidences of anastomotic, rectal and mesorectal, pelvic presacral space, abdominal presacral space, internal iliac node, external iliac node, obturator node, inguinal node, and ischiorectal fossa recurrences were 42.5% (57/134), 26.9% (36/134), 25.4% (34/134), 7.5% (10/134), 34.3% (46/134), 3.7% (5/134), 0.7% (1/134), 9.7% (13/134), and 8.2% (11/134), respectively. Compared with mid- lower rectal cancer, upper rectal cancer was more prone to metastasis in the abdominal presacral space (19.0% vs. 5.6%, P=0.028). Patients with inguinal lymph node metastasis were more likely to harbor external iliac node metastasis (23.1% vs. 1.7%, P=0.006). Conclusions There is a great difference in the recurrence patterns between upper and mid-lower rectal cancer. As a result, the clinical target volumes of radiation therapy for upper and mid-lower rectal cancer should be defined separately. Optimizing the clinical target volume of radiotherapy will be of great value in the future. -
Key words:
- rectal cancer /
- tumor recurrence /
- radiotherapy /
- target volume design
-

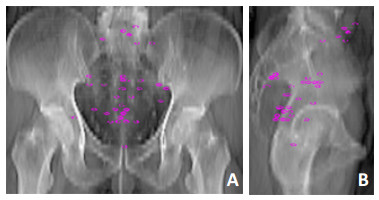
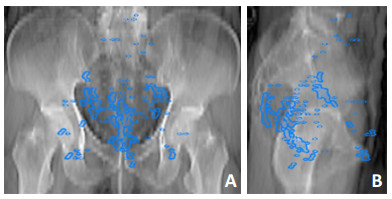
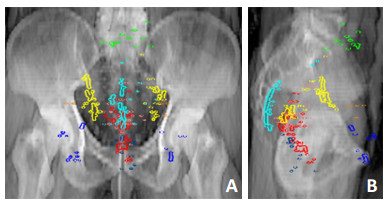
图 1 134例患者盆腔复发位置分布图
绿色:骶前淋巴引流区腹部组;红色:吻合口;粉色:直肠残端、术区及周围区域;黄色:髂内淋巴引流区;浅蓝色:骶前淋巴引流盆腔组;橙色:髂外淋巴引流区;紫色:闭孔淋巴引流区;宝蓝色:腹股沟淋巴引流区;深蓝色:坐骨直肠窝
A:正位图;B:侧位图表 1 134例直肠癌术后盆腔区域复发患者临床资料

表 2 134例不同分段直肠癌术后复发部位比例

表 3 134例不同病理分期下直肠癌术后复发部位比例

表 4 髂外淋巴引流区转移与腹股沟淋巴引流区转移相关性检验

表 5 骶前淋巴引流区腹部组转移患者资料统计

-
[1] Huguier M, Houry S. Treatment of local recurrence of rectal cancer [J]. Am J Surg, 1998, 175(4):288-292. doi: 10.1016/S0002-9610(98)00016-6 [2] Kusters M, Marijnen CA, van de Velde CJ, et al. Patterns of local recurrence in rectal cancer: a study of the Dutch TME trial[J]. Eur J Surg Oncol, 2010, 36(5):470-476. doi: 10.1016/j.ejso.2009.11.011 [3] Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phaseⅢ trial after a median follow- up of 11 years[J]. J Clin Oncol, 2012, 30(16):1926- 1933. doi: 10.1200/JCO.2011.40.1836 [4] Breugom AJ, Swets M, Bosset JF, et al. Adjuvant chemotherapy after preoperative (chemo)radiotherapy and surgery for patients with rectal cancer: a systematic review and meta-analysis of individual patient data[J]. Lancet Oncol, 2015, 16(2):200-207. doi: 10.1016/S1470-2045(14)71199-4 [5] Roels S, Duthoy W, Haustermans K, et al. Definition and delineation of the clinical target volume for rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2006, 65(4):1129-1142. doi: 10.1016/j.ijrobp.2006.02.050 [6] Samuelian JM, Callister MD, Ashman JB, et al. Reduced acute bowel toxicity in patients treated with intensity-modulated radiotherapy for rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2012, 82(5): 1981-1987. doi: 10.1016/j.ijrobp.2011.01.051 [7] Valentini V, Gambacorta MA, Barbaro B, et al. International consensus guidelines on clinical target volume delineation in rectal cancer [J]. Radiat Oncol, 2016, 120(2):195-201. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=3594946087097ae46c81412d951638cc [8] Glimelius B, Gronberg H, Jarhult J, et al. A systematic overview of radiation therapy effects in rectal cancer[J]. Acta Oncol, 2003, 42(5-6):476-492. doi: 10.1080/02841860310012301 [9] Birgisson H, Pahlman L, Gunnarsson U, et al. Late adverse effects of radiation therapy for rectal cancer: A systematic overview[J]. Acta Oncol, 2007, 46(4):504-516. doi: 10.1080/02841860701348670 [10] 任骅, 金晶, 肖琴, 等.直肠癌术前IMRT同期化疗与VMAT同期化疗的急性不良反应比较[J].中华放射肿瘤学杂志, 2014, 23(3):205- 209. doi: 10.3760/cma.j.issn.1004-4221.2014.03.007 [11] 唐源, 金晶, 朱远, 等.直肠癌术前/术后适形/调强放疗放疗靶区勾画共识与图谱[J].中华放射肿瘤学杂志, 2018, 27(3):227-234. doi: 10.3760/cma.j.issn.1004-4221.2018.03.001 [12] Syk E, Torkzad MR, Blomqvist L, et al. Local recurrence in rectal cancer:anatomic localization and effect on radiation target[J]. Int J Radiat Oncol Biol Phys, 2008, 72(3):658-664. doi: 10.1016/j.ijrobp.2008.01.063 [13] Nijkamp J, Kusters M, Beets-Tan RG, et al. Three dimensional analysis of recurrence patterns in rectal cancer: the cranial border in hypofractionated preoperative radiotherapy can be lowered[J]. Int J Radiat Oncol Biol Phys, 2011, 80(1):103-110. doi: 10.1016/j.ijrobp.2010.01.046 [14] 胡祥.直肠淋巴引流系统的局部解剖和分类[J].中国实用外科杂志, 2018, 38(10):1128-1132. http://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK201810009.htm [15] Steup WH, Moriya Y, van de Velde CJ, et al. Patterns of lymphatic spread in rectal cancer. A topographical analysis on lymph node metastases[J]. Eur J Cancer, 2002, 38(7):911-918. doi: 10.1016/S0959-8049(02)00046-1 [16] Bell S, Sasaki J, Sinclair G, et al. Understanding the anatomy of lymphatic drainage and the use of blue-dye mapping to determine the extent of lymphadenectomy in rectal cancer surgery: unresolved issues[J]. Colorectal Dis, 2009, 11(5):443-449. doi: 10.1111/cdi.2009.11.issue-5 -

 下载:
下载:
 点击查看大图
点击查看大图
图(5) / 表(5)
计量
- 文章访问数: 66
- HTML全文浏览量: 5
- PDF下载量: 4
- 被引次数: 0
