
Selection strategy for complete cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy among patients with gastric cancer with peritoneal metastasis
-
摘要:
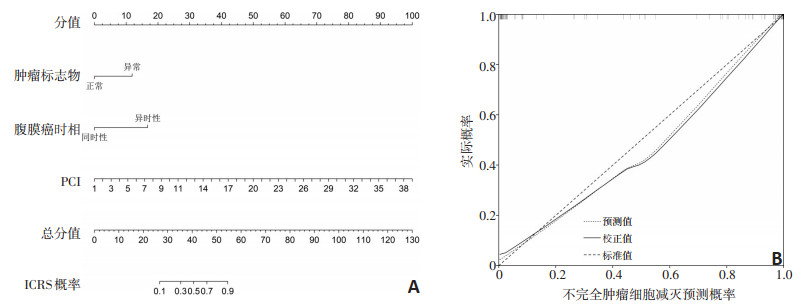
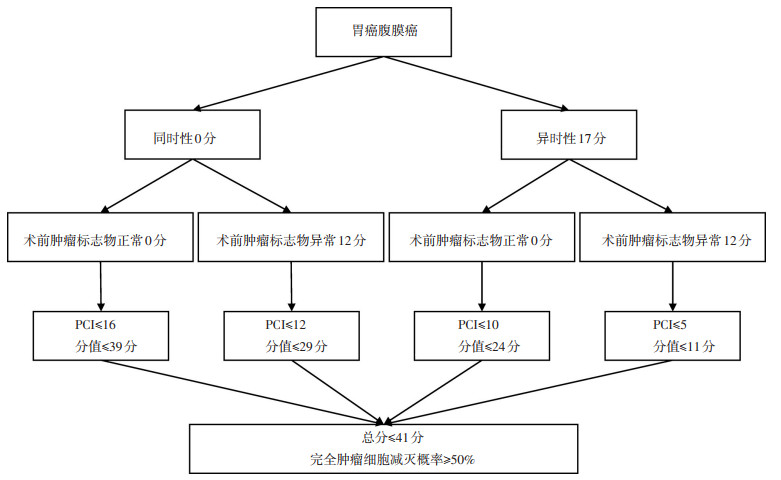
目的 构建肿瘤细胞减灭程度(completeness of cytoreduction,CC)预测模型,为肿瘤细胞减灭术(cytoreductive surgery,CRS)加腹腔热灌注化疗(hyperthermic intraperitoneal chemotherapy,HIPEC)治疗胃癌腹膜转移(gastric cancer with peritoneal metastasis,GCPM)提供病例筛选方法。 方法 比较完全CRS(complete CRS,CCRS)组和不完全CRS(incomplete CRS,ICRS)组患者基本临床病理特征和治疗参数,通过逻辑回归模型筛选CC独立预测因子,精准预测CCRS可能性。 结果 125例患者纳入本研究,其中CC0组52例(41.6%),中位总生存期为30.0(95% CI:16.8~43.3)个月;CC1-3组73例,中位总生存期7.3(95% CI:5.7~8.8)个月,差异有统计学意义(P < 0.001),而CC1、CC2和CC3组间中位总生存期差异无统计学意义(P>0.05)。因此,CC0定义为CCRS组,CC1-3定义为ICRS组,构建并优化了以腹膜转移时相(OR=14,95% CI:2.0~97.9,P=0.008)、术前肿瘤标志物(OR=6.5,95% CI:2.1~37.8,P=0.037)和腹膜癌指数(OR=1.5,95% CI:1.3~1.8,P < 0.001)预测ICRS的多因素回归模型和预测列线图,内部验证显示,ROC曲线下面积为0.985,列线图显示预测准确度、一致性良好。根据列线图结果将患者分为4个亚组,设定CCRS预测概率≥ 50%,同时性且术前肿瘤标志物正常组、同时性且术前肿瘤标志物异常组、异时性且术前肿瘤标志物正常组、异时性且术前肿瘤标志物异常组腹膜癌指数界值点分别为:≤ 16、≤ 12、≤ 10和≤ 5。 结论 CCRS+HIPEC可延长部分经选择的GCPM患者生存期,以腹膜癌指数为核心,联合腹膜转移时相和术前肿瘤标志物的病例筛选策略,可有效选择高概率实现CCRS的患者接受CCRS+HIPEC治疗。 Abstract:Objective To construct a predictive model to assess the completeness of cytoreduction (CC) and help guiding selection for cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy (CRS+HIPEC) in patients with gastric cancer with peritoneal metastasis (GCPM). Methods GCPM patients treated with CRS+HIPEC at Beijing Shijitan Hospital were enrolled in this study. The major clinicopathologic and therapeutic characteristics were compared between those with complete CRS (CCRS) and incomplete CRS (ICRS). A nomogram based on a Logistic regression model was constructed for predicting the risk of ICRS. The nomogram was evaluated using area under receiver operating characteristic curve (AUC) and validated using the bootstrap resampling method. The probability of CCRS was predicted using the nomogram. Results Among the included 125 patients with GCPM, 52 had CC0 cytoreduction and 73 had CC1-3 cytoreduction. The median overall survival (mOS) was 30.0 (95% CI: 16.8-43.3) months in the CC0 group, which was significantly longer than the mOS of 7.3 (95% CI: 5.8- 8.8) months in the CC1- 3 group (P < 0.001). As there were no significant differences in OS among the CC1, CC2, and CC3 groups, CC0 patients were included in the CCRS group and CC1-3 patients were included in the ICRS group. Multivariate Logistic regression demonstrated that the time of peritoneal metastasis development (OR=14, 95% CI: 2.0-97.9, P= 0.008), preoperative tumor markers (TM) (OR=6.5, 95% CI: 2.1-37.8, P=0.037), and peritoneal cancer index (PCI) (OR=1.5, 95% CI: 1.3- 1.8, P < 0.001) were independent predictive factors for ICRS. The AUC of the nomogram was 0.985. Internal validation displayed good accuracy and consistency between the predictions and the actual observations. The cutoffs of PCI, with the probability of CCRS set at ≥ 50%, were ≤16, ≤12, ≤10, and ≤5 for synchronous GCPM with normal TM, synchronous GCPM with abnormal TM, metachronous GCPM with normal TM, and metachronous GCPM with abnormal TM, respectively. Conclusions Complete CRS+HIPEC improves the survival of some patients with GCPM. A selection strategy based on PCI combined with the time of peritoneal metastasis development and TM may be a practical way for selecting patients with GCPM eligible for CCRS. -
表 1 CCRS与ICRS组基本临床病理特征比较

表 2 ICRS风险的逻辑回归分析

-
[1] Ji ZH, Peng KW, Yu Y, et al. Current status and future prospects of clinical trials on CRS+HIPEC for gastric cancer peritoneal metastases[J]. Int J Hyperthermia, 2017, 33(5):562-570. doi: 10.1080/02656736.2017.1283065 [2] 季加孚, 沈琳, 徐惠绵, 等.胃癌腹膜转移防治中国专家共识[J].中国医学前沿杂志(电子版), 2017, 9(5):29-40. http://d.old.wanfangdata.com.cn/Periodical/zjyx201715001 [3] Lambert LA. Looking up:Recent advances in understanding and treating peritoneal carcinomatosis[J]. CA Cancer J Clin, 2015, 65(4):284-298. http://cn.bing.com/academic/profile?id=e881900992c729dd26bfcf7c29f1ddb5&encoded=0&v=paper_preview&mkt=zh-cn [4] 李雁, 许洪斌, 彭正, 等.肿瘤细胞减灭术加腹腔热灌注化疗治疗腹膜假黏液瘤专家共识[J].中华医学杂志, 2019, 99(20):1527-1535. doi: 10.3760/cma.j.issn.0376-2491.2019.20.003 [5] Li Y, Zhou YF, Liang H, et al. Chinese expert consensus on cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal malignancies[J]. World J Gastroenterol, 2016, 22(30):6906-6916. http://cn.bing.com/academic/profile?id=f6a2362edfad8c95518f231029e8719c&encoded=0&v=paper_preview&mkt=zh-cn [6] Bonnot PE, Piessen G, Kepenekian V, et al. Cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy for gastric cancer with peritoneal metastases (CYTO-CHIP study):A propensity score analysis[J]. J Clin Oncol, 2019, 37(23):2028-2040. http://cn.bing.com/academic/profile?id=7f5d435389358fefd035b2a7c5a6883c&encoded=0&v=paper_preview&mkt=zh-cn [7] 姬忠贺, 李鑫宝, 刘刚, 等.肿瘤细胞减灭术加腹腔热灌注化疗治疗110例胃癌腹膜癌临床分析[J].中华医学杂志, 2018, 98(38):3097-3083. http://d.old.wanfangdata.com.cn/Periodical/zhyx201838007 [8] Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis[J]. Cancer Treat Res, 1996, 82:359-374. http://cn.bing.com/academic/profile?id=499678730f63a644f609bdab5e5bbfad&encoded=0&v=paper_preview&mkt=zh-cn [9] Sugarbaker PH. Cytoreductice surgery & perioperative chemotherapy for peritoneal surface malignancy[M]. Second ed. Woodbury: CineMed Inc, 2017: 207-219. [10] Yonemura Y, Prabhu A, Sako S, et al. Long term survival after cytoreductive surgery combined with perioperative chemotherapy in gastric cancer patients with peritoneal metastasis[J]. Cancers (Basel), 2020, 12(1):116. doi: 10.3390/cancers12010116 [11] Yang XJ, Huang CQ, Suo T, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer:final results of a phase Ⅲ randomized clinical trial[J]. Ann Surg Oncol, 2011, 18(6):1575-1581. doi: 10.1245/s10434-011-1631-5 [12] Glehen O, Schreiber V, Cotte E, et al. Cytoreductive surgery and intraperitoneal chemohyperthermia for peritoneal carcinomatosis arising from gastric cancer[J]. Arch Surg, 2004, 139(1):20-26. http://cn.bing.com/academic/profile?id=274a873820545ccbb7002e7b4c68067c&encoded=0&v=paper_preview&mkt=zh-cn [13] Ji ZH, Sun JH, Wu HT, et al. Assessment of hyperthermic intraperitoneal chemotherapy to eradicate intraperitoneal free cancer cells[J]. Transl Oncol, 2016, 9(1):18-24. http://cn.bing.com/academic/profile?id=af6a016fb0eab9c3326bf16836f11350&encoded=0&v=paper_preview&mkt=zh-cn [14] Glehen O, Gilly FN, Arvieux C, et al. Peritoneal carcinomatosis from gastric cancer:a multi-institutional study of 159 patients treated by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy[J]. Ann Surg Oncol, 2010, 17(9):2370-2377. doi: 10.1245/s10434-010-1039-7 [15] Wang Y, Li J, Xia Y, et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy[J]. J Clin Oncol, 2013, 31(9):1188-1195. doi: 10.1200/JCO.2012.41.5984 [16] Coccolini F, Catena F, Glehen O, et al. Complete versus incomplete cytoreduction in peritoneal carcinosis from gastric cancer, with consideration to PCI cut-off. Systematic review and meta-analysis[J]. Eur J Surg Oncol, 2015, 41(7):911-919. doi: 10.1016/j.ejso.2015.03.231 -

 下载:
下载:

 点击查看大图
点击查看大图

图(4) / 表(2)
计量
- 文章访问数: 148
- HTML全文浏览量: 6
- PDF下载量: 17
- 被引次数: 0
