
Analysis of screening methods for DNA mismatch repair gene deletion in colorectal cancer
-
摘要:
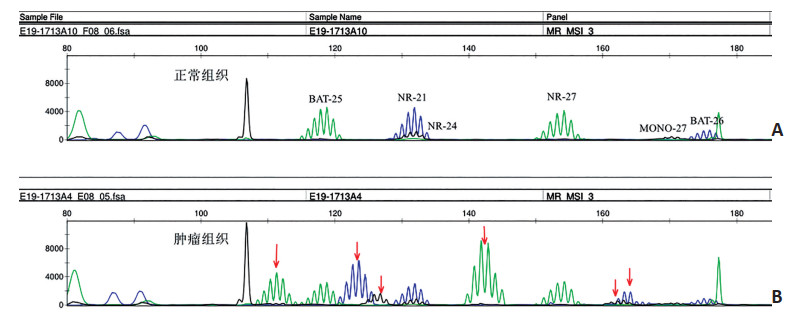
目的 通过对筛查结直肠癌DNA错配修复(mismatch repair,MMR)基因缺失两种最常用的检测方法的分析,寻找更为经济有效的检测策略。 方法 分析新疆医科大学第一附属医院2018年9月至2019年9月收治并行手术的结直肠癌患者的肿瘤组织223例,采用免疫组织化学法检测平台检测MLH1、MSH2、PMS2、MSH6的表达缺失情况,PCR-毛细管电泳法检测肿瘤微卫星不稳定(microstatellites instability,MSI)状态。 结果 在223例结直肠癌中,27例(12.1%)MMR蛋白表达缺失(MMR deficiency,dMMR),196例(87.9%)MMR蛋白表达完整(MMR proficient,pMMR)。MLH1、MSH2、MSH6和PMS2的缺失率分别为9.0%(20/223)、1.8%(4/223)、2.7%(6/223)和9.4%(21/223)。包含PMS2和MSH6的2种抗体试验筛查dMMR结直肠癌的灵敏度和特异度与4种抗体试验(MLH1、MSH2、PMS2、MSH6)的灵敏度和特异度均相同。微卫星高度不稳定(MSI-high,MSI-H)27例(12.1%),微卫星稳定(microsatellite stable,MSS)196例(87.9%),无微卫星低度不稳定(MSI-low,MSI-L)。BAT-25、BAT-26、NR-21、NR-24、NR-27、MONO-27共6个位点的灵敏度分别为88.9%、92.6%、96.3%、70.4%、92.6%、77.8%。将MSI定义为3种标记(NR-21、NR-27、BAT-26)至少有1处不稳定时,得出的结果与6种标记组(BAT-25、BAT-26、NR-21、NR-24、NR-27、MONO-27)完全相同。 结论 简化的两种检测方案为结直肠癌dMMR/MSI的鉴定提供了更为简便、可靠、价格低廉的方法。 Abstract:Objective Here, we aimed to analyze the two most commonly used methods for screening DNA mismatch repair (MMR) gene deletions in colorectal cancer to establish a more cost-effective strategy. Methods A total of 223 patients with colorectal cancer were recruited from the First Affiliated Hospital of Xinjiang Medical University for this study from September 2018 to September 2019. Using the Ventana BenchMark ULTRA automatic immunohistochemistry platform, the expression levels of MLH1, MSH2, PMS2, and MSH6 proteins were assessed, and the microsatellite instability (MSI) status of the tumors was then determined through PCR capillary electrophoresis. Results Among the 223 patients with colorectal cancer, 27 (12.1%) had MMR deficiency (dMMR) and 196 (87.9%) had MMR proficiency (pMMR). The missing rates of MLH1, MSH2, MSH6, and PMS2 were estimated as 9.0% (20/223), 1.8% (4/223), 2.7% (6/223), and 9.4% (21/223), respectively. The sensitivity and specificity of the two-antibody test employing antibodies against only PMS2 and MSH6 for screening dMMR colorectal cancer were the same as those of the four-antibody test. Twenty-seven cases exhibited high microsatellite instability (MSI-H) (12.1%) and 196 cases exhibited microsatellite stability (MSS) (87.9%). However, no case exhibited low microsatellite stability (MSI-L). The sensitivities of BAT-25, BAT-26, NR-21, NR-24, NR-27, and MONO-27 were 88.9%, 92.6%, 96.3%, 70.4%, 92.6%, and 77.8%, respectively. When MSI was defined using three markers, NR-21, NR-27, and BAT-26, with at least one of the three exhibiting instability, the results were the same as those obtained using the six-marker group. Conclusions The proposed two-marker detection strategy provides a simple, reliable, and low-cost method for the identification of dMMR/MSI in colorectal cancer. -
Key words:
- colorectal cancer /
- DNA mismatch repair /
- microsatellite instability
-
表 1 微卫星状态与临床病理特征的相关性

表 2 两种免疫组织化学法预测结直肠癌MSI的比较
例(%) 
表 3 两种MSI检测方案检测MMR蛋白表达的比较
例(%) 
-
[1] Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China[J]. Chin J Cancer Res, 2018, 30(1):1-12. doi: 10.21147/j.issn.1000-9604.2018.01.01 [2] Tariq K, Ghias K. Colorectal cancer carcinogenesis:a review of mechanisms[J]. Cancer Biol Med, 2016, 13(1):120-135. doi: 10.20892/j.issn.2095-3941.2015.0103 [3] Hampel H, Frankel WL, Martin E, et al. Feasibility of screening for Lynch syndrome among patients with colorectal cancer[J]. J Clin Oncol, 2008, 26(35):5783-5788. doi: 10.1200/JCO.2008.17.5950 [4] 王雯邈, 董林, 李文斌, 等.Lynch综合征相关结直肠癌的遗传基因及分子病理筛查策略[J].中华结直肠疾病电子杂志, 2018, 7(2):176-180. doi: 10.3877/cma.j.issn.2095-3224.2018.02.015 [5] Hechtman JF, Middha S, Stadler ZK, et al. Universal screening for microsatellite instability in colorectal cancer in the clinical genomics era:new recommendations, methods, and considerations[J]. Fam Cancer, 2017, 16(4):525-529. doi: 10.1007/s10689-017-9993-x [6] Dienstmann R, Mason MJ, Sinicrope FA, et al. Prediction of overall survival in stage Ⅱ and Ⅲ colon cancer beyond TNM system:a retrospective, pooled biomarker study[J]. Ann Oncol, 2017, 28(5):1023-1031. doi: 10.1093/annonc/mdx052 [7] Venderbosch S, Nagtegaal ID, Maughan TS, et al. Mismatch repair status and BRAF mutation status in metastatic colorectal cancer patients:a pooled analysis of the CAIRO, CAIRO2, COIN, and FOCUS studies[J]. Clin Cancer Res, 2014, 20(20):5322-5330. doi: 10.1158/1078-0432.CCR-14-0332 [8] Le DT, Uram JN, Wang H, et al. PD-1 Blockade in Tumors with MismatchRepair Deficiency[J]. N Engl J Med, 2015, 72(26):2509-2520. https://www.ncbi.nlm.nih.gov/pubmed/26559583 [9] Le DT, Durham JN, Smith KN, et al. Mismatch-repair deficiency predicts response of solid tumors to PD-1 blockade[J]. Science, 2017, 357(6349):409-413. doi: 10.1126/science.aan6733 [10] Overman MJ, Lonardi S, Wong KYM, et al. Durable clinical benefit with nivolumab plus ipilimumabin DNA mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer[J]. J Clin Oncol, 2018, 36(8):773-779. doi: 10.1200/JCO.2017.76.9901 [11] Truninger K, Menigatti M, Luz J, et al. Immunohistochemical analysis reveals high frequency of PMS2 defects in colorectal cancer[J]. Gastroenterology, 2005, 128(5):1160-1171. doi: 10.1053/j.gastro.2005.01.056 [12] Cheah PL, Li J, Looi LM, et al. Screening for microsatellite instability in colorectal carcinoma:practical utility of immunohistochemistry and PCR with fragment analysis in a diagnostic histopathology setting[J]. Malays J Pathol, 2019, 41(2):91-100. http://cn.bing.com/academic/profile?id=e02654ac24380a55f4dc8a34ca1fa0e0&encoded=0&v=paper_preview&mkt=zh-cn [13] Goshayeshi L, Khooiee A, Ghaffarzadegan K, et al. Screening for Lynchsyndrome in cases with colorectal carcinoma from Mashhad[J]. Arch IranMed, 2017, 20(6):332-337. https://pubmed.ncbi.nlm.nih.gov/28646840/ [14] Yan WY, Hu J, Xie L, et al. Prediction of biological behavior and prognosis of colorectal cancer patients by tumor MSI/MMR in the Chinese population[J]. Onco Targets Ther, 2016, 9:7415-7424. doi: 10.2147/OTT.S117089 [15] 胡晓儒, 徐灿, 亢野, 等.658例结直肠癌错配修复蛋白的表达及其与临床病理特征的关系[J].中华病理学杂志, 2018, 47(11):827-833. doi: 10.3760/cma.j.issn.0529-5807.2018.11.003 [16] Kevans D, Wang LM, Sheahan K, et al. Epithelial-mesenchymal transition (emt) protein expression in a cohort of stageⅡ colorectal cancer patients with characterized tumor budding and mismatch repair protein status[J]. Int J Surg Pathol, 2011, 19(6):751-760. doi: 10.1177/1066896911414566 [17] Leicher LW, Lammertink MHA, Offerman SR, et al. Consequences of testing for mismatch repair deficiency of colorectal cancer in clinical practice[J]. Scand J Gastroenterol, 2018, 53(5):632-636. doi: 10.1080/00365521.2017.1406534 [18] Evrard C, Tachon G, Randrian V, et al. Microsatellite instability:Diagnosis, heterogeneity, discordance, and clinical impact in colorectal cancer[J]. Cancers, 2019, 11(10):1567. doi: 10.3390/cancers11101567 [19] Mathews NS, Masih D, Mittal R, et al. Microsatellite instability in young patients with mucinous colorectal cancers-characterization using molecular testing, immunohistochemistry, and histological features[J]. Indian J Cancer, 2019, 56(4):309-314. doi: 10.4103/ijc.IJC_224_18 [20] Pastrello C, Baglioni S, Tibiletti MG, et al. Stability of BAT26 in tumours of hereditary nonpolyposis colorectal cancer patients with MSH2 intragenic deletion[J]. Eur J Hum Genet, 2006, 14(1):63-68. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=1c592155ddfc011c5f373f3a7bf39738 [21] Goel A, Nagasaka T, Hamelin R, et al. An optimized pentaplex PCR for detecting DNA mismatch repair-deficient colorectal cancers[J]. PLoS One, 2010, 5(2):e9393. doi: 10.1371/journal.pone.0009393 -

 下载:
下载:
 点击查看大图
点击查看大图

图(2) / 表(3)
计量
- 文章访问数: 155
- HTML全文浏览量: 20
- PDF下载量: 8
- 被引次数: 0
