
Second generation sequencing detection breast cancer susceptibility gene variants for risk prediction and clinical treatment
-
摘要:目的 通过二代测序技术筛选乳腺癌易感基因突变位点,探讨其对乳腺癌风险预测、临床干预及预后指导的意义。方法 采取2013年11月至2015年7月272例就诊天津医科大学肿瘤医院的乳腺癌患者146例、高危人群71例及健康者55例3组样本的外周血,采用二代测序技术进行DNA检测。采用Amplicon方法筛选BRCA1、BRCA2、PTEN、STK11、TP53及BAP1全外显子区域有价值的突变位点,分析3组的基因突变发生率及乳腺癌患者易感基因突变与临床病理特征之间的相关性。结果 经筛选获得177个突变位点,去重后共得到67个突变位点,其中包括50个单核苷酸突变(single nucleotide variants,SNVs)、8个无义突变(non-sense mutation)和9个插入缺失突变(insertion-deletions,InDels)。3组突变位点中31个突变位点收录于ExAC数据库,40个突变位点收录于Clin Var数据库。本研究中21个新发现的突变位点在ExAC、Clin Var或db SNP数据库中均未提及。统计分析发现85.1%(57/67)的突变发生于乳腺癌患者及高危人群中,且突变阳性乳腺癌患者有较高的淋巴结转移率(P=0.010)及病理分期(P=0.002),致病性突变的乳腺癌患者的肿瘤家族史(P=0.005)及三阴性乳腺癌比例(P=0.009)均高于非致病性突变者。结论 乳腺癌易感基因突变位点在乳腺癌风险预测、临床治疗及预后评价方面具有重要意义。Abstract:Objective To investigate the function of breast cancer susceptibility gene variants in predicting breast cancer risk and guiding clinical treatment through DNA sequencing.Methods This study involved 146 patients, 71 high-risk cases, and 55 healthy people, totaling 272 cases. The subjects were treated in Tianjin Medical University Cancer Institute and Hospital from November 2013 to July 2015. Genomic DNA was sequenced by a second generation sequencing platform. All exon areas of six common breast cancer susceptibility genes (BRCA1, BRCA2, PTEN, STK11, TP53, and RAP1) were sequenced through amplicon sequencing method. Meaningful variants including single nucleotide variants (SNVs), insertion-deletions (InDels) and nonsense mutations were selected and statistical methods, such as t test and χ2 test, were used to analyze the statistical differences in incidence rates among three groups. Results: A total of 177 meaningful variants were confirmed, including 50 SNVs, 8 nonsense mutations, and 9 InDels. Among the variants, 31 were recorded in the Exome Aggregation Consortium (ExAC), 40 were noted in ClinVar database, and 21 were not encoded in the present database, which were defined as new variants in this study. Conversely, 57 variants (85.1%) were found in breast cancer patients and high-risk cases, and the incidence of axillary lymph node metastasis (P=0.010) and pathological stages (P=0.002) in mutation positive patients were both higher than mutation negative patients. Moreover, the percentage of family history of cancer (P=0.005) and triple negative breast cancer (P=0.009) were both higher in patients carrying pathogenic mutations than in nonpathogenic patients.Conclusion Breast cancer susceptibility gene variants may not only be a tool used to predict the risk of getting breast cancer but also a meaningful guideline for the clinical treatment and prognosis evaluation.
-
乳腺癌早期预防是其发病率降低的主要原因[1]。流行病学调查显示,乳腺癌易感基因突变主要表现在其家族的聚集性[2],其中二代测序技术对检测乳腺癌易感基因突变具有重要意义。本研究旨在对BRCA1、BRCA2、PTEN、TP53、STK11和BAP1乳腺癌易感基因进行测序,分析其在乳腺癌风险预测、临床治疗及预后评价中的意义。
1. 材料与方法
1.1 材料
1.1.1 病例资料
采取2013年11月至2015年7月272例于天津医科大学肿瘤医院诊治的146例乳腺癌患者、71例高危人群及55例健康者的外周血。入选标准:1)患者:同意入组的乳腺癌患者;2)高危人群:既往有肿瘤病史(已排除皮肤基底细胞癌、宫颈原位癌等早期癌)或家族中2位及以上一级亲属患恶性肿瘤(年龄≤50岁);3)健康人群:既往无肿瘤病史及肿瘤家族史。本研究得到天津医科大学肿瘤医院伦理委员会批准,且患者均签署知情同意书。
1.1.2 试剂
Control DNA ACD1、Control Oligo Pool ACP1、CAT、OHS1、SW1、UB1、TDP1/PMM2 PCR扩增预混液、LNA1/LNB1混合试剂、NW1均购自美国Illu-mina公司。
1.2 方法
1.2.1 标本采集
采取患者外周静脉血5 mL,1 200 r/min离心10 min后,取中间悬浮层白膜200 μL。
1.2.2 DNA提取
吸取20 μL蛋白酶K、200 μL全血样本及200 μL缓冲液AL至1.5 mL离心管混匀,56℃孵育10 min,短暂离心后加入200 μL无水乙醇混匀,8 000 r/min离心1 min,弃滤液。分别加入500 μL缓冲液AW1、AW2混匀,8 000 r/min及14 000 r/min短暂离心后,加入200 μL缓冲液AE,室温孵育1 min,8 000 r/min离心1 min。
1.2.3 DNA浓度及纯度测量
初始化仪器后,取1.5 μL去离子水作为空白对照,依次加入1.2 μL的DNA提取样本检测其OD值,保留OD260/280为1.8~2.0、浓度为50 ng/μL及以上的样本。
1.2.4 DNA文库制备
实验方法参照美国Illumina公司的TruSeq Amplicon Cancer Panel说明书操作[3]。
1.2.5 突变位点致病性检测
通过SIFT、Polyphen2、LRT、Mutation Taster、Mutation Assessor、FATHMM、Meta SVM和Meta LR软件对筛选出的每一个突变位点进行检测。当有1个软件预测某个突变位点为功能缺陷时记为1分,通过ROC曲线得出能够预测致病性突变的cut off值为2.5分。本研究将3组样本中突变位点评分≥3分时定为致病性突变,对于插入缺失突变(insertion-deletions,InDels)和无义突变(non-sense mutation)采用Mutation Taster进行评价。
1.3 统计学分析
采用SPSS 20.0软件进行统计学分析。计量资料采用t检验;计数资料采用χ2检验。P<0.05为差异具有统计学意义。
2. 结果
2.1 样本测序数据的质量统计
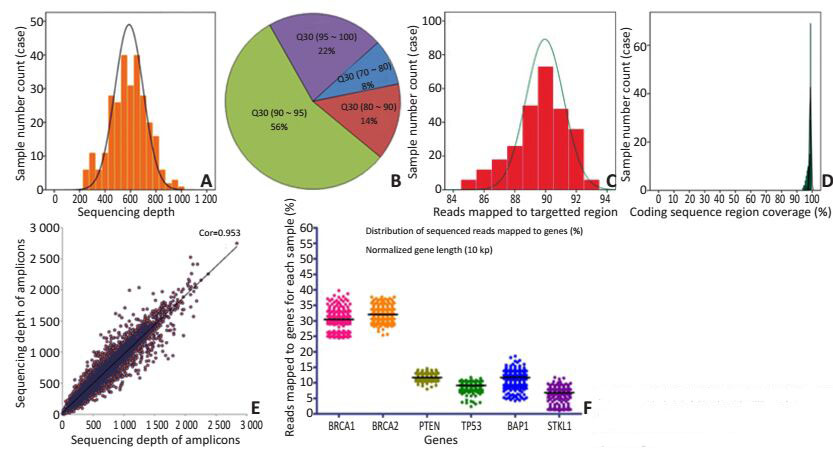
3组样本测序深度为200~1 000×(图 1A);92%样本的Q30超过80%(图 1B);读取至目标区域的数据超过85%(图 1C);编码区的覆盖率达到95%以上(图 1D);样本间测序深度保持一致(图 1E);不同基因所占数据量比例稳定(图 1F)。
![]() 图 1 样本测序数据的质量统计(A~F)Figure 1. The data quality statistics of sequencing samples (A~F)
图 1 样本测序数据的质量统计(A~F)Figure 1. The data quality statistics of sequencing samples (A~F)2.2 样本突变位点的筛选流程
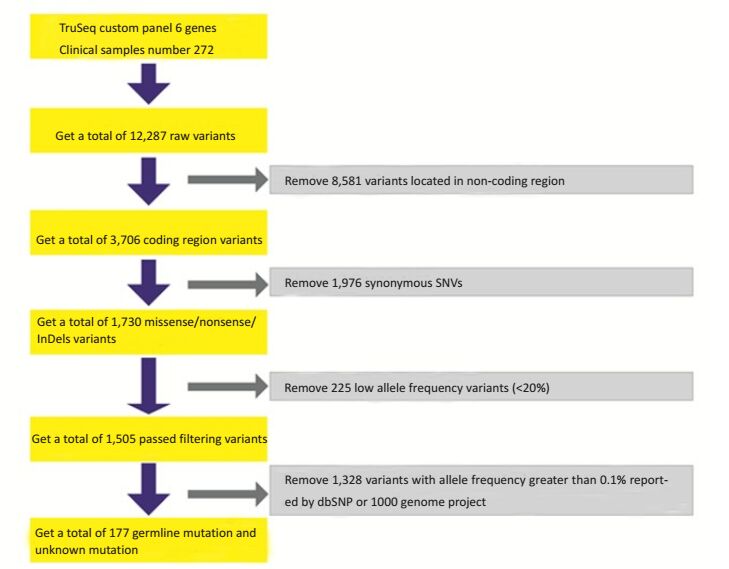
通过图 2所示筛选的方式共获得177个突变位点,其中包含158个单核苷酸突变(single nucleotide variants,SNVs)、8个无义突变和11个InDels。去重后为67个突变位点,包括50个SNVs、8个无义突变和9个InDels。突变位点与ExAC、ClinVar数据库收录相同的为31、40个,本研究新发现的21个突变位点在ExAC,Clin Var或dbSNP数据库中均未提及。
2.3 乳腺癌易感基因突变分布及风险预测
本研究最终发现的67个基因突变中50个(74.6%)发生于BRCA1/2,46个分别收录于ExAC,ClinVar或dbSNP数据库。46个突变中22个(47.8%)为致病性突变,其中5个为InDels、6个为无义突变、11个为错义突变。本研究新发现的21个突变位点中14个(66.7%)为致病性突变,其中3个为InDels、2个为无义突变、9个为错义突变。
2.4 检测样本中乳腺癌易感基因的分布情况
本研究行外周血检测的272例患者中携带突变的为164例,其中乳腺癌患者70例、高危人群49例、健康者45例。乳腺癌患者的突变位点为42个,高危人群为22个,健康者为10个,高达85.1%(57/67)突变发生于乳腺癌患者及高危人群。146例乳腺癌患者中9例临床病理资料缺失,137例乳腺癌患者中易感基因突变及易感基因致病性突变与临床病理特征的关系见表 1。
表 1 6个乳腺癌易感基因突变及易感基因致病性突变与乳腺癌患者临床病理特征的关系Table 1. Relationship of breast cancer susceptibility gene mutation and pathologic mutation with clinicopathologic feature of patients
3. 讨论
研究表明乳腺癌易感基因突变是乳腺癌具有家族聚集性的重要原因[4],其中BRCA1/2是较为重要的两个基因,携带BRCA1/2突变的70岁前健康女性罹患乳腺癌的累计风险高达55%~85%[5],TP53、PTEN、STK11、CDH1、ATM、CHEK2乳腺癌易感基因也与乳腺癌发生发展密切相关[6]。
本研究通过二代测序技术筛选乳腺癌易感基因全外显子区域突变位点,与传统的一代测序相比二代测序的优势是更加高效[7]。目前,乳腺癌易感基因检测因缺乏热点区,所检测的基因片段较长,选择传统的检测技术效果不佳,因此二代测序技术备受瞩目。同时,二代测序技术也存在不足之处,如检测步骤较繁琐,数据分析难度大,并且存在大量未知位点的判读等。基于以上优缺点,二代测序技术仍得到国内外学者的广泛应用[8-9]。本研究测序结果中得出测序数据质量高、目标区域测序深度均匀、目标区域覆盖度好、扩增效率稳定、样本间测序深度重复性高、样本间碱基变化分布均匀、突变图谱符合Germ-line Mutation特征的优势。
本研究通过筛选得到67个突变位点,其中46个突变(68.7%)收录于ExAC、ClinVar或dbSNP数据库,由此证实本研究结果的可信度,21个突变位点(31.3%)为本研究中新发现的突变位点,且均发生于乳腺癌患者或高危人群,由此说明这些新发现的突变位点可作为预测乳腺癌发病风险的新切入点,为进一步的研究提供理论依据。统计分析发现,乳腺癌易感基因突变在乳腺癌患者及高危人群中的发生率为85.1%(57/67),明显高于健康者的1.5%(1/67),提示检测乳腺癌易感基因突变位点可为预测乳腺癌发生风险、提高早期乳腺癌的检出率提供帮助。但需要指出的是,筛选出的突变位点需要更多的研究来验证,从而建立安全有效的乳腺癌危险预测模型,达到指导乳腺癌危险评估的目的。
本研究进一步分析发现,突变阳性患者的腋下淋巴结转移比例较高(P=0.010),且病理分期中Ⅲ期患者所占比例较大(P=0.002),由此提示发生易感基因突变的乳腺癌患者预后可能更差,对携带乳腺癌易感基因突变患者需要考虑是否适当强化临床治疗。研究表明,BRCA1突变的乳腺癌中高达70%患者为三阴性乳腺癌,BRCA2突变的乳腺癌中16%~ 23%患者为三阴性乳腺癌[10],本研究发现在6个乳腺癌易感基因突变的患者中致病性突变患者的三阴性乳腺癌所占比例高(P=0.009),与上述研究结果一致。
综上所述,本研究通过二代测序技术检测乳腺癌易感基因突变情况,从而为乳腺癌早期预防,临床治疗及预后评价提供一定理论依据,但由于本研究样本例数较少,且未进行相关生存分析,因此其对于乳腺癌患者治疗及预后的指导意义有待进一步证实。
-
![]()
图 1 样本测序数据的质量统计(A~F)
Figure 1. The data quality statistics of sequencing samples (A~F)
表 1 6个乳腺癌易感基因突变及易感基因致病性突变与乳腺癌患者临床病理特征的关系
Table 1 Relationship of breast cancer susceptibility gene mutation and pathologic mutation with clinicopathologic feature of patients
 下载: 导出CSV
下载: 导出CSV
-
[1] Hooks MA. Breast cancer: risk assessment and prevention[J]. South Med J, 2010, 103(4):333-338. DOI: 10.1097/SMJ.0b013e3181d39038
[2] Collaborative Group on Hormonal Factors in Breast Cancer. Familial breast cancer: collaborative reanalysis of individual data from 52 epidemiological studies including 58, 209 women with breast cancer and 101, 986 women without the disease[J]. Lancet, 2001, 358 (9291):1389-1399. DOI: 10.1016/S0140-6736(01)06524-2
[3] Simen BB, Yin L, Goswami CP, et al. Validation of a next-generationsequencing cancer panel for use in the clinical laboratory[J]. Arch Pathol Lab Med, 2015, 139(4):508-517. DOI: 10.5858/arpa.2013-0710-OA
[4] Hedenfalk IA, Ringnér M, Trent JM, et al. Gene expression in inherited breast cancer[J]. Adv Cancer Res, 2002, 84:1-34. DOI: 10.1016/S0065-230X(02)84001-5
[5] Hall MJ, Reid JE, Burbidge LA, et al. BRCA1 and BRCA2 mutations in women of different ethnicities undergoing testing for hereditary breast-ovarian cancer[J]. Cancer, 2009, 115(10):2222-2233. DOI: 10.1002/cncr.24200
[6] Zhang B, Beeghly-Fadiel A, Long J, et al. Genetic variants associated with breast-cancer risk: comprehensive research synopsis, metaanalysis, and epidemiological evidence[J]. Lancet Oncol, 2011, 12(5): 477-488. DOI: 10.1016/S1470-2045(11)70076-6
[7] Hong H, Zhang W, Shen J, et al. Critical role of bioinformatics in translating huge amounts of next-generation sequencing data into personalized medicine[J]. Sci China Life Sci, 2013, 56(2):110-118. DOI: 10.1007/s11427-013-4439-7
[8] Jalkh N, Chouery E, Haidar Z, et al. Next-generation sequencing in familial breast cancer patients from Lebanon[J]. BMC Med Genomics, 2017, 10(1):8. DOI: 10.1186/s12920-017-0244-7
[9] Kluska A, Balabas A, Paziewska A, et al. New recurrent BRCA1/2 mutations in Polish patients with familial breast/ovarian cancer detected by next generation sequencing[J]. BMC Med Genomics, 2015, 8:19. DOI: 10.1186/s12920-015-0092-2
[10] Stevens KN, Vachon CM, Couch FJ. Genetic susceptibility to triplenegative breast cancer[J]. Cancer Res, 2013, 73(7):2025-2030. DOI: 10.1158/0008-5472.CAN-12-1699
-
期刊类型引用(2)
1. 李富,曾健. 基因检测在乳腺癌综合治疗中的应用现状及进展. 广西医科大学学报. 2021(02): 408-412 .  百度学术
百度学术
2. 吕德明,俎彩霞,吕凌霄. 乳腺癌PTEN、Ki-67、Bcl-2和BRCA-1蛋白表达情况及其与临床预后的关系. 中国妇幼保健. 2020(10): 1921-1924 . 百度学术
其他类型引用(2)
计量
- 文章访问数: 54
- HTML全文浏览量: 42
- PDF下载量: 9
- 被引次数: 4
